
Page 50 - Read Online
P. 50
Page 4 of 14 Zhang et al. Vessel Plus 2021;5:48 https://dx.doi.org/10.20517/2574-1209.2021.64
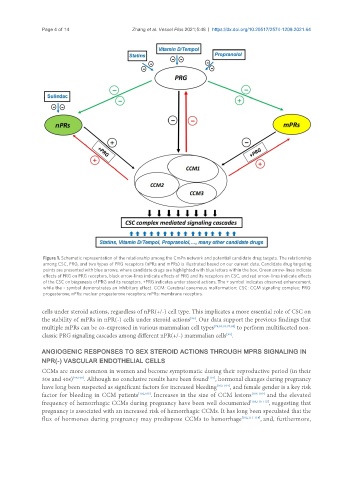
Figure 1. Schematic representation of the relationship among the CmPn network and potential candidate drug targets. The relationship
among CSC, PRG, and two types of PRG receptors (nPRs and mPRs) is illustrated based on our current data. Candidate drug targeting
points are presented with blue arrows, where candidate drugs are highlighted with blue letters within the box. Green arrow-lines indicate
effects of PRG on PRG receptors, black arrow-lines indicate effects of PRG and its receptors on CSC, and red arrow-lines indicate effects
of the CSC on biogenesis of PRG and its receptors. +PRG indicates under steroid actions. The + symbol indicates observed enhancement,
while the - symbol demonstrates an inhibitory effect. CCM: Cerebral cavernous malformation; CSC: CCM signaling complex; PRG:
progesterone; nPRs: nuclear progesterone receptors; mPRs: membrane receptors.
cells under steroid actions, regardless of nPR(+/-) cell type. This implicates a more essential role of CSC on
the stability of mPRs in nPR(-) cells under steroid actions . Our data support the previous findings that
[96]
multiple mPRs can be co-expressed in various mammalian cell types [78,83,93,97,98] to perform multifaceted non-
classic PRG signaling cascades among different nPR(+/-) mammalian cells .
[93]
ANGIOGENIC RESPONSES TO SEX STEROID ACTIONS THROUGH MPRS SIGNALING IN
NPR(-) VASCULAR ENDOTHELIAL CELLS
CCMs are more common in women and become symptomatic during their reproductive period (in their
30s and 40s) [99,100] . Although no conclusive results have been found , hormonal changes during pregnancy
[101]
have long been suspected as significant factors for increased bleeding [102-104] , and female gender is a key risk
factor for bleeding in CCM patients [102,105] . Increases in the size of CCM lesions [106-109] and the elevated
frequency of hemorrhagic CCMs during pregnancy have been well documented [103,110-115] , suggesting that
pregnancy is associated with an increased risk of hemorrhagic CCMs. It has long been speculated that the
flux of hormones during pregnancy may predispose CCMs to hemorrhage [102,111-114] , and, furthermore,