
Page 57 - Read Online
P. 57
Ashenhurst et al. Vessel Plus 2024;8:3 https://dx.doi.org/10.20517/2574-1209.2023.90 Page 11 of 15
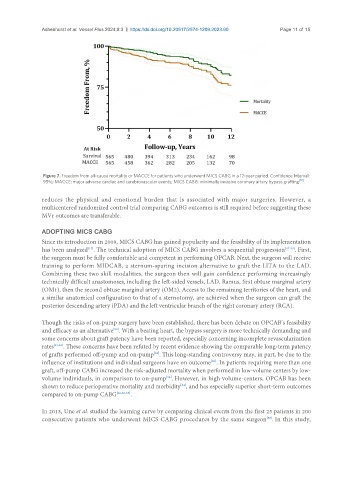
Figure 7. Freedom from all-cause mortality or MACCE for patients who underwent MICS CABG in a 12-year period. Confidence Interval:
95%; MACCE: major adverse cardiac and cerebrovascular events; MICS CABG: minimally invasive coronary artery bypass grafting [18] .
reduces the physical and emotional burden that is associated with major surgeries. However, a
multicentered randomized control trial comparing CABG outcomes is still required before suggesting these
MVr outcomes are transferable.
ADOPTING MICS CABG
Since its introduction in 2009, MICS CABG has gained popularity and the feasibility of its implementation
[17]
has been analyzed . The technical adoption of MICS CABG involves a sequential progression [47-49] . First,
the surgeon must be fully comfortable and competent in performing OPCAB. Next, the surgeon will receive
training to perform MIDCAB, a sternum-sparing incision alternative to graft the LITA to the LAD.
Combining these two skill modalities, the surgeon then will gain confidence performing increasingly
technically difficult anastomoses, including the left-sided vessels, LAD, Ramus, first obtuse marginal artery
(OM1), then the second obtuse marginal artery (OM2). Access to the remaining territories of the heart, and
a similar anatomical configuration to that of a sternotomy, are achieved when the surgeon can graft the
posterior descending artery (PDA) and the left ventricular branch of the right coronary artery (RCA).
Though the risks of on-pump surgery have been established, there has been debate on OPCAB’s feasibility
and efficacy as an alternative . With a beating heart, the bypass surgery is more technically demanding and
[50]
some concerns about graft patency have been reported, especially concerning incomplete revascularization
rates [51,52] . These concerns have been refuted by recent evidence showing the comparable long-term patency
of grafts performed off-pump and on-pump . This long-standing controversy may, in part, be due to the
[53]
influence of institutions and individual surgeons have on outcome . In patients requiring more than one
[50]
graft, off-pump CABG increased the risk-adjusted mortality when performed in low-volume centers by low-
volume individuals, in comparison to on-pump . However, in high volume-centers, OPCAB has been
[54]
[54]
shown to reduce perioperative mortality and morbidity , and has especially superior short-term outcomes
compared to on-pump CABG [28,52-55] .
In 2013, Une et al. studied the learning curve by comparing clinical events from the first 25 patients in 200
consecutive patients who underwent MICS CABG procedures by the same surgeon . In this study,
[56]