
Page 196 - Read Online
P. 196
Page 8 of 16 Harik et al. Vessel Plus 2023;7:30 https://dx.doi.org/10.20517/2574-1209.2023.124
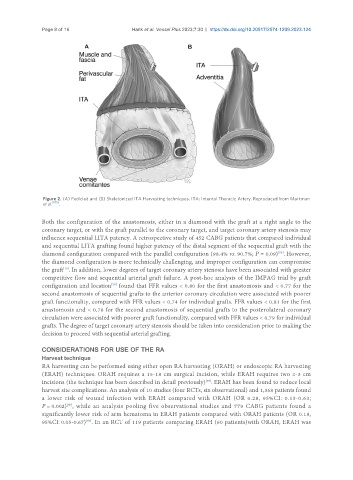
Figure 2. (A) Pedicled and (B) Skeletonized ITA Harvesting techniques. ITA: Internal Thoracic Artery. Reproduced from Markman
et al. [105] .
Both the configuration of the anastomosis, either in a diamond with the graft at a right angle to the
coronary target, or with the graft parallel to the coronary target, and target coronary artery stenosis may
influence sequential LITA patency. A retrospective study of 452 CABG patients that compared individual
and sequential LITA grafting found higher patency of the distal segment of the sequential graft with the
[56]
diamond configuration compared with the parallel configuration (98.4% vs. 90.7%; P = 0.09) . However,
the diamond configuration is more technically challenging, and improper configuration can compromise
[10]
the graft . In addition, lower degrees of target coronary artery stenosis have been associated with greater
competitive flow and sequential arterial graft failure. A post-hoc analysis of the IMPAG trial by graft
configuration and location found that FFR values < 0.80 for the first anastomosis and < 0.77 for the
[58]
second anastomosis of sequential grafts to the anterior coronary circulation were associated with poorer
graft functionality, compared with FFR values < 0.74 for individual grafts. FFR values < 0.81 for the first
anastomosis and < 0.78 for the second anastomosis of sequential grafts to the posterolateral coronary
circulation were associated with poorer graft functionality, compared with FFR values < 0.79 for individual
grafts. The degree of target coronary artery stenosis should be taken into consideration prior to making the
decision to proceed with sequential arterial grafting.
CONSIDERATIONS FOR USE OF THE RA
Harvest technique
RA harvesting can be performed using either open RA harvesting (ORAH) or endoscopic RA harvesting
(ERAH) techniques. ORAH requires a 15-18 cm surgical incision, while ERAH requires two 2-3 cm
[59]
incisions (the technique has been described in detail previously) . ERAH has been found to reduce local
harvest site complications. An analysis of 10 studies (four RCTs, six observational) and 1,368 patients found
a lower risk of wound infection with ERAH compared with ORAH (OR 0.28, 95%CI: 0.13-0.63;
[60]
P = 0.002) , while an analysis pooling five observational studies and 779 CABG patients found a
significantly lower risk of arm hematoma in ERAH patients compared with ORAH patients (OR 0.18,
95%CI: 0.05-0.67) . In an RCT of 119 patients comparing ERAH (60 patients)with ORAH, ERAH was
[60]