
Page 112 - Read Online
P. 112
Page 8 of 11 Flattery et al. Vessel Plus 2024;8:26 https://dx.doi.org/10.20517/2574-1209.2023.130
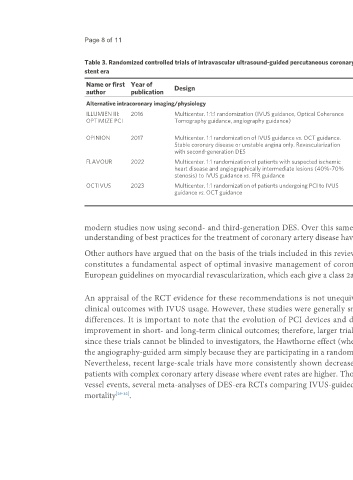
Table 3. Randomized controlled trials of intravascular ultrasound-guided percutaneous coronary intervention compared with alternative imaging or physiology assessments in the drug-eluting
stent era
Name or first Year of Design Size Primary endpoint Clinical outcomes
author publication
Alternative intracoronary imaging/physiology
ILLUMIEN III: 2016 Multicenter. 1:1:1 randomization (IVUS guidance, Optical Coherence 450 Primary efficacy: post-PCI minimum stent No significant difference in post-PCI minimum stent
OPTIMIZE PCI Tomography guidance, angiography guidance) area (assessed by OCT) area between groups. No significant in procedural or
Primary safety: procedural MACE 30-day MACE between groups
OPINION 2017 Multicenter. 1:1 randomization of IVUS guidance vs. OCT guidance. 817 TVF (cardiac death, target-vessel related No significant difference in rates of any primary or
Stable coronary disease or unstable angina only. Revascularization MI, ischemia-driven TVR) secondary outcomes between groups at 12 months
with second-generation DES
FLAVOUR 2022 Multicenter. 1:1 randomization of patients with suspected ischemic 1,682 Composite of death from any cause, MI, or No significant difference in event rates or patient-
heart disease and angiographically intermediate lesions (40%-70% any revascularization reported symptoms (SAQ score) at 24 months
stenosis) to IVUS guidance vs. FFR guidance between groups
OCTIVUS 2023 Multicenter. 1:1 randomization of patients undergoing PCI to IVUS 2,008 Composite of death from cardiac causes, No significant difference in event rates between
guidance vs. OCT guidance target vessel-related MI, or ischemia-driven study groups
TVR at 1 year
modern studies now using second- and third-generation DES. Over this same period, medical therapy for coronary artery disease and the medical field’s
understanding of best practices for the treatment of coronary artery disease have similarly matured.
Other authors have argued that on the basis of the trials included in this review, as well as meta-analyses and registry data, intravascular imaging during PCI
constitutes a fundamental aspect of optimal invasive management of coronary artery disease [1,2,4,5] . This perspective is supported in both American and
European guidelines on myocardial revascularization, which each give a class 2a recommendation to IVUS guidance in PCI in their most recent iterations [3,28] .
An appraisal of the RCT evidence for these recommendations is not unequivocally positive; many early studies in this space showed no improvement in
clinical outcomes with IVUS usage. However, these studies were generally smaller and potentially underpowered to detect small but clinically significant
differences. It is important to note that the evolution of PCI devices and drugs has resulted in a steady decrease in procedural adverse events and an
improvement in short- and long-term clinical outcomes; therefore, larger trials were needed to demonstrate the benefit of intravascular imaging. Moreover,
since these trials cannot be blinded to investigators, the Hawthorne effect (whereby the investigators perform more optimized PCI in patients randomized to
the angiography-guided arm simply because they are participating in a randomized trial) likely narrows the difference between the two randomized strategies.
Nevertheless, recent large-scale trials have more consistently shown decreased incidence of MACE with the addition of IVUS to PCI, particularly among
patients with complex coronary artery disease where event rates are higher. Though the benefit in individual trials has been typically limited to reducing target-
vessel events, several meta-analyses of DES-era RCTs comparing IVUS-guided with angiography-only PCI have demonstrated a reduction in cardiovascular
mortality [29-32] .