
Page 159 - Read Online
P. 159
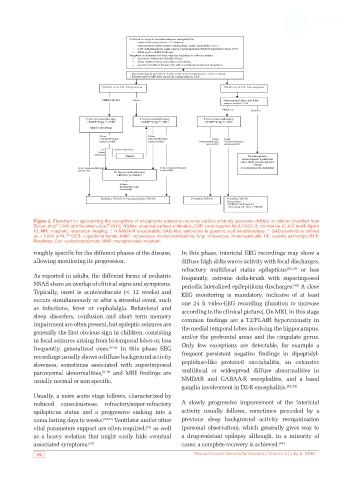
Figure 2. Flowchart for approaching the recognition of encephalitis related to neuronal surface antibody syndrome (NSAS) in children [modified from
[8]
[1]
Zuliani et al. 2012 and Suleiman et al. 2013]. NSAbs: neuronal surface antibodies; CSF: cerebrospinal fluid; CXCL13: chemokine (C-X-C motif) ligand
13; MRI: magnetic resonance imaging; *: in NMDA-R encephalitis; GAD-Abs: antibodies to glutamic acid decarboxylase; *: GAD positivity is defined
[8]
as > 1,000 u/mL. OCB: oligoclonal bands; IvMP: intravenous methylprednisolone; IvIg: intravenous immunoglobulin; PE: plasma exchange; RTX:
Rituximab; Cyc: cyclophosphamide; MMF: mycophenolate mophetil.
roughly specific for the different phases of the disease, In this phase, interictal EEG recordings may show a
allowing monitoring its progression. diffuse high delta waves activity with focal discharges,
refractory multifocal status epilepticus [38,39] or less
As reported in adults, the different forms of pediatric frequently, extreme delta-brush with superimposed
NSAS share an overlap of clinical signs and symptoms. periodic lateralized epileptiform discharges. A close
[39]
Typically, onset is acute/subacute (< 12 weeks) and EEG monitoring is mandatory, inclusive of at least
occurs simultaneously or after a stressful event, such one 24 h video-EEG recording (duration to increase
as infections, fever or cephalalgia. Behavioral and according to the clinical picture). On MRI, in this stage
sleep disorders, confusion and short term memory common findings are a T2/FLAIR hyperintensity in
impairment are often present, but epileptic seizures are the medial temporal lobes involving the hippocampus,
generally the first obvious sign in children, consisting
in focal seizures arising from bi-temporal lobes or, less and/or the prefrontal areas and the cingulate gyrus.
frequently, generalized ones. [8-10] In this phase EEG Only few exceptions are detectable, for example a
recordings usually shows a diffuse background activity frequent persistent negative findings in dipeptidyl-
slowness, sometimes associated with superimposed peptidase-like protein-6 encephalitis, an extensive
paroxysmal abnormalities, [9,39] and MRI findings are multifocal or widespread diffuse abnormalities in
usually normal or non specific. NMDAR and GABAA-R encephalitis, and a basal
ganglia involvement in D2-R encephalitis. [42,43]
Usually, a more acute stage follows, characterized by
reduced consciousness, refractory/super-refractory A slowly progressive improvement of the interictal
epilepticus status and a progressive sinking into a activity usually follows, sometimes preceded by a
coma lasting days to weeks. [40,41] Ventilator and/or other previous sleep background activity reorganization
[13]
vital parameters support are often required, as well (personal observation), which generally gives way to
as a heavy sedation that might easily hide eventual a drug-resistant epilepsy although, in a minority of
associated symptoms. [28] cases, a complete recovery is achieved. [44]
150 Neuroimmunol Neuroinflammation | Volume 3 | July 8, 2016