
Page 33 - Read Online
P. 33
Mokhtar et al. Laparoscopic rectosigmoidopexy for intractable rectal prolapse in children
Optic port (5 mm)
Working ports (5 mm)
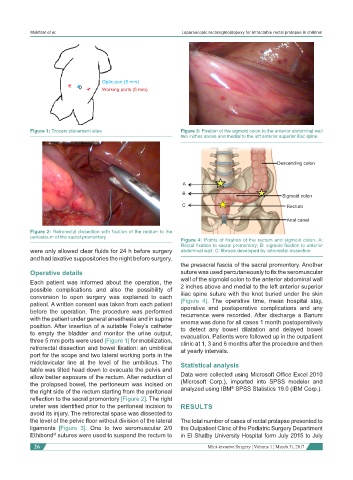
Figure 1: Trocars placement sites Figure 3: Fixation of the sigmoid colon to the anterior abdominal wall
two inches above and medial to the left anterior superior iliac spine
Descending colon
A
B Sigmoid colon
C Rectum
Anal canal
Figure 2: Retrorectal dissection with fixation of the rectum to the
periosteum of the sacral promontory
Figure 4: Points of fixation of the rectum and sigmoid colon. A:
Rectal fixation to sacral promontory; B: sigmoid fixation to anterior
were only allowed clear fluids for 24 h before surgery abdominal wall; C: fibrosis developed by retrorectal dissection
and had laxative suppositories the night before surgery.
the presacral fascia of the sacral promontory. Another
Operative details suture was used percutaneously to fix the seromuscular
Each patient was informed about the operation, the wall of the sigmoid colon to the anterior abdominal wall
possible complications and also the possibility of 2 inches above and medial to the left anterior superior
conversion to open surgery was explained to each iliac spine suture with the knot buried under the skin
patient. A written consent was taken from each patient [Figure 4]. The operative time, mean hospital stay,
before the operation. The procedure was performed operative and postoperative complications and any
recurrence were recorded. After discharge a Barium
with the patient under general anesthesia and in supine enema was done for all cases 1 month postoperatively
position. After insertion of a suitable Foley’s catheter to detect any bowel dilatation and delayed bowel
to empty the bladder and monitor the urine output, evacuation. Patients were followed up in the outpatient
three 5 mm ports were used [Figure 1] for mobilization, clinic at 1, 3 and 6 months after the procedure and then
retrorectal dissection and bowel fixation: an umbilical at yearly intervals.
port for the scope and two lateral working ports in the
midclavicular line at the level of the umbilicus. The Statistical analysis
table was tilted head down to evacuate the pelvis and
allow better exposure of the rectum. After reduction of Data were collected using Microsoft Office Excel 2010
the prolapsed bowel, the peritoneum was incised on (Microsoft Corp.), imported into SPSS modeler and
®
the right side of the rectum starting from the peritoneal analyzed using IBM SPSS Statistics 19.0 (IBM Corp.).
reflection to the sacral promontory [Figure 2]. The right
ureter was identified prior to the peritoneal incision to RESULTS
avoid its injury. The retrorectal space was dissected to
the level of the pelvic floor without division of the lateral The total number of cases of rectal prolapse presented to
ligaments [Figure 3]. One to two seromuscular 2/0 the Outpatient Clinic of the Pediatric Surgery Department
Ethibond sutures were used to suspend the rectum to in El Shatby University Hospital form July 2015 to July
®
26 Mini-invasive Surgery ¦ Volume 1 ¦ March 31, 2017