
Page 41 - Read Online
P. 41
Page 4 of 14 Abe et al. Mini-invasive Surg 2023;7:28 https://dx.doi.org/10.20517/2574-1225.2023.15
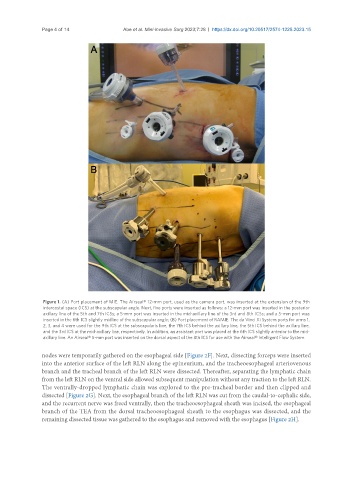
Figure 1. (A) Port placement of MIE. The Airseal® 12-mm port, used as the camera port, was inserted at the extension of the 9th
intercostal space (ICS) at the subscapular angle. Next, five ports were inserted as follows: a 12-mm port was inserted in the posterior
axillary line of the 5th and 7th ICSs; a 5-mm port was inserted in the mid-axillary line of the 3rd and 8th ICSs; and a 5-mm port was
inserted in the 6th ICS slightly midline of the subscapular angle; (B) Port placement of RAMIE. The da Vinci Xi System ports for arms 1,
2, 3, and 4 were used for the 9th ICS at the subscapularis line, the 7th ICS behind the axillary line, the 5th ICS behind the axillary line,
and the 3rd ICS at the mid-axillary line, respectively. In addition, an assistant port was placed at the 6th ICS slightly anterior to the mid-
axillary line. An Airseal® 5-mm port was inserted on the dorsal aspect of the 8th ICS for use with the Airseal® Intelligent Flow System.
nodes were temporarily gathered on the esophageal side [Figure 2F]. Next, dissecting forceps were inserted
into the anterior surface of the left RLN along the epineurium, and the tracheoesophageal arteriovenous
branch and the tracheal branch of the left RLN were dissected. Thereafter, separating the lymphatic chain
from the left RLN on the ventral side allowed subsequent manipulation without any traction to the left RLN.
The ventrally-dropped lymphatic chain was explored to the pre-tracheal border and then clipped and
dissected [Figure 2G]. Next, the esophageal branch of the left RLN was cut from the caudal-to-cephalic side,
and the recurrent nerve was freed ventrally, then the tracheoesophageal sheath was incised, the esophageal
branch of the TEA from the dorsal tracheoesophageal sheath to the esophagus was dissected, and the
remaining dissected tissue was gathered to the esophagus and removed with the esophagus [Figure 2H].