
Page 91 - Read Online
P. 91
Thinagaran et al. Mini-invasive Surg 2021;5:46 https://dx.doi.org/10.20517/2574-1225.2021.53 Page 5 of 18
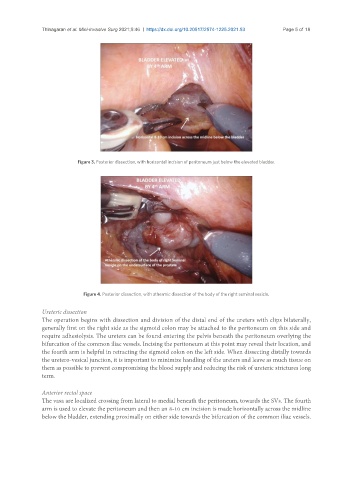
Figure 3. Posterior dissection, with horizontal incision of peritoneum just below the elevated bladder.
Figure 4. Posterior dissection, with athermic dissection of the body of the right seminal vesicle.
Ureteric dissection
The operation begins with dissection and division of the distal end of the ureters with clips bilaterally,
generally first on the right side as the sigmoid colon may be attached to the peritoneum on this side and
require adhesiolysis. The ureters can be found entering the pelvis beneath the peritoneum overlying the
bifurcation of the common iliac vessels. Incising the peritoneum at this point may reveal their location, and
the fourth arm is helpful in retracting the sigmoid colon on the left side. When dissecting distally towards
the uretero-vesical junction, it is important to minimize handling of the ureters and leave as much tissue on
them as possible to prevent compromising the blood supply and reducing the risk of ureteric strictures long
term.
Anterior rectal space
The vasa are localized crossing from lateral to medial beneath the peritoneum, towards the SVs. The fourth
arm is used to elevate the peritoneum and then an 8-10 cm incision is made horizontally across the midline
below the bladder, extending proximally on either side towards the bifurcation of the common iliac vessels.