
Page 78 - Read Online
P. 78
Gharagozloo et al. Mini-invasive Surg 2020;4:66 I http://dx.doi.org/10.20517/2574-1225.2020.53 Page 19 of 22
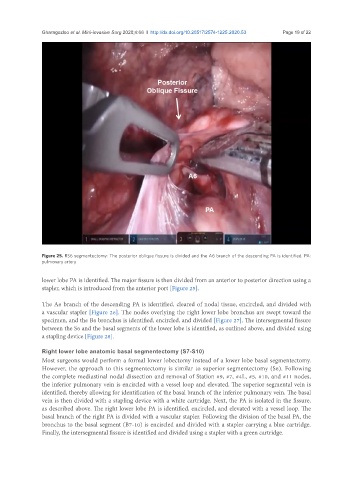
Figure 25. RS6 segmentectomy: The posterior oblique fissure is divided and the A6 branch of the descending PA is identified. PA:
pulmonary artery
lower lobe PA is identified. The major fissure is then divided from an anterior to posterior direction using a
stapler, which is introduced from the anterior port [Figure 25].
The A6 branch of the descending PA is identified, cleared of nodal tissue, encircled, and divided with
a vascular stapler [Figure 26]. The nodes overlying the right lower lobe bronchus are swept toward the
specimen, and the B6 bronchus is identified, encircled, and divided [Figure 27]. The intersegmental fissure
between the S6 and the basal segments of the lower lobe is identified, as outlined above, and divided using
a stapling device [Figure 28].
Right lower lobe anatomic basal segmentectomy (S7-S10)
Most surgeons would perform a formal lower lobectomy instead of a lower lobe basal segmentectomy.
However, the approach to this segmentectomy is similar to superior segmentectomy (S6). Following
the complete mediastinal nodal dissection and removal of Station #9, #7, #4L, #5, #10, and #11 nodes,
the inferior pulmonary vein is encircled with a vessel loop and elevated. The superior segmental vein is
identified, thereby allowing for identification of the basal branch of the inferior pulmonary vein. The basal
vein is then divided with a stapling device with a white cartridge. Next, the PA is isolated in the fissure,
as described above. The right lower lobe PA is identified, encircled, and elevated with a vessel loop. The
basal branch of the right PA is divided with a vascular stapler. Following the division of the basal PA, the
bronchus to the basal segment (B7-10) is encircled and divided with a stapler carrying a blue cartridge.
Finally, the intersegmental fissure is identified and divided using a stapler with a green cartridge.