
Page 32 - Read Online
P. 32
Page 8 of 13 Gharagozloo et al. Mini-invasive Surg 2020;4:55 I http://dx.doi.org/10.20517/2574-1225.2020.42
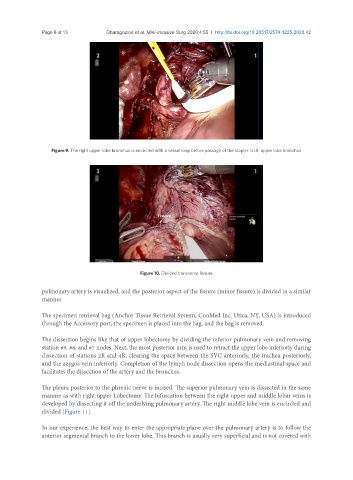
Figure 9. The right upper lobe bronchus is encircled with a vessel loop before passage of the stapler. ULB: upper lobe bronchus
Figure 10. Divided transverse fissure
pulmonary artery is visualized, and the posterior aspect of the fissure (minor fissure) is divided in a similar
manner.
The specimen retrieval bag (Anchor Tissue Retrieval System, ConMed Inc. Utica, NY, USA) is introduced
through the Accessory port, the specimen is placed into the bag, and the bag is removed.
The dissection begins like that of upper lobectomy by dividing the inferior pulmonary vein and removing
station #9, #8, and #7 nodes. Next, the most posterior arm is used to retract the upper lobe inferiorly during
dissection of stations 2R and 4R, clearing the space between the SVC anteriorly, the trachea posteriorly,
and the azygos vein inferiorly. Completion of the lymph node dissection opens the mediastinal space and
facilitates the dissection of the artery and the bronchus.
The pleura posterior to the phrenic nerve is incised. The superior pulmonary vein is dissected in the same
manner as with right upper Lobectomy. The bifurcation between the right upper and middle lobar veins is
developed by dissecting it off the underlying pulmonary artery. The right middle lobe vein is encircled and
divided [Figure 11].
In our experience, the best way to enter the appropriate plane over the pulmonary artery is to follow the
anterior segmental branch to the lower lobe. This branch is usually very superficial and is not covered with