
Page 59 - Read Online
P. 59
Page 6 of 9 Shiozaki et al. Mini-invasive Surg 2020;4:50 I http://dx.doi.org/10.20517/2574-1225.2020.31
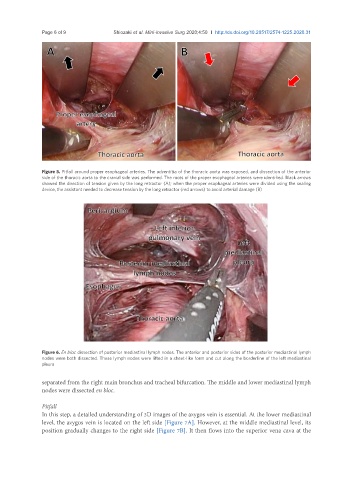
Figure 5. Pitfall around proper esophageal arteries. The adventitia of the thoracic aorta was exposed, and dissection of the anterior
side of the thoracic aorta to the cranial side was performed. The roots of the proper esophageal arteries were identified. Black arrows
showed the direction of tension given by the long retractor (A); when the proper esophageal arteries were divided using the sealing
device, the assistant needed to decrease tension by the long retractor (red arrows) to avoid arterial damage (B)
Figure 6. En bloc dissection of posterior mediastinal lymph nodes. The anterior and posterior sides of the posterior mediastinal lymph
nodes were both dissected. These lymph nodes were lifted in a sheet-like form and cut along the borderline of the left mediastinal
pleura
separated from the right main bronchus and tracheal bifurcation. The middle and lower mediastinal lymph
nodes were dissected en bloc.
Pitfall
In this step, a detailed understanding of 3D images of the azygos vein is essential. At the lower mediastinal
level, the azygos vein is located on the left side [Figure 7A]. However, at the middle mediastinal level, its
position gradually changes to the right side [Figure 7B]. It then flows into the superior vena cava at the