
Page 20 - Read Online
P. 20
Hashida et al. Mini-invasive Surg 2024;8:14 https://dx.doi.org/10.20517/2574-1225.2023.139 Page 3 of 8
Table 1. Effects of elevated abdominal air pressures summarized by high and low airway pressure
Airway pressure Abdominal air pressure CVP Possibility to control bleeding
High ↑↑ ↑↑↑ Impossible
Medium (usual pressure) ↑↑ ↑ Possible
Extremely low ↑↑ ↑ ↓ Possible (high risk of gas embolism)
The arrows indicate the relative increase (↑) or decrease (↓) in pressure levels. CVP: Central venous pressure.
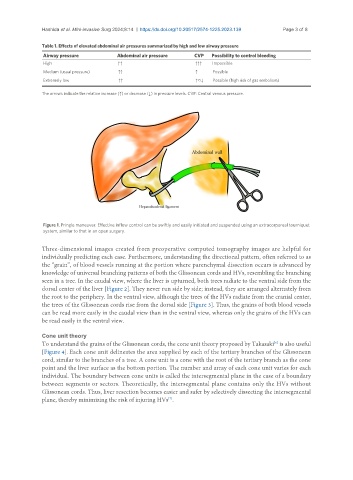
Figure 1. Pringle maneuver. Effective inflow control can be swiftly and easily initiated and suspended using an extracorporeal tourniquet
system, similar to that in an open surgery.
Three-dimensional images created from preoperative computed tomography images are helpful for
individually predicting each case. Furthermore, understanding the directional pattern, often referred to as
the “grain”, of blood vessels running at the portion where parenchymal dissection occurs is advanced by
knowledge of universal branching patterns of both the Glissonean cords and HVs, resembling the branching
seen in a tree. In the caudal view, where the liver is upturned, both trees radiate to the ventral side from the
dorsal center of the liver [Figure 2]. They never run side by side; instead, they are arranged alternately from
the root to the periphery. In the ventral view, although the trees of the HVs radiate from the cranial center,
the trees of the Glissonean cords rise from the dorsal side [Figure 3]. Thus, the grains of both blood vessels
can be read more easily in the caudal view than in the ventral view, whereas only the grains of the HVs can
be read easily in the ventral view.
Cone unit theory
To understand the grains of the Glissonean cords, the cone unit theory proposed by Takasaki is also useful
[6]
[Figure 4]. Each cone unit delineates the area supplied by each of the tertiary branches of the Glissonean
cord, similar to the branches of a tree. A cone unit is a cone with the root of the tertiary branch as the cone
point and the liver surface as the bottom portion. The number and array of each cone unit varies for each
individual. The boundary between cone units is called the intersegmental plane in the case of a boundary
between segments or sectors. Theoretically, the intersegmental plane contains only the HVs without
Glissonean cords. Thus, liver resection becomes easier and safer by selectively dissecting the intersegmental
plane, thereby minimizing the risk of injuring HVs .
[7]