
Page 146 - Read Online
P. 146
McKenna et al Hypoxia in prostate cancer
Table 2: HAPs which have been tested in human clinical trials
Prodrug Company or institution Chemical class Mechanism of cytotoxicity References
Tirapazamine (SR 4233) SRI International/NCI Aromatic N-oxide Complex DNA damage [102,103]
Apaziquone (E09) Spectrum Quinone DNA interstrand crosslink [104,105]
Evofosfamide TH-302 Threshold Nitroaromatic DNA interstrand crosslink [106-108]
Tarloxitinib Threshold and University of Nitroaromatic Pan-HER inhibitor [109]
TH-4000 Auckland Tyrosine kinase inhibitor
PR-104 Proacta and University of Nitroaromatic DNA interstrand crosslink [110,111]
Auckland
Banoxantrone (AQ4N) KuDOS/Novacea Aliphatic N-oxide DNA intercalator and topo II [35]
inhibitor
Porfiromycin Vion Pharmaceuticals Quinone DNA interstrand crosslink [112,113]
RH1 CRUK Quinone DNA interstrand crosslink [114]
NCI: National Cancer Institute; CRUK: Cancer Research UK; HER: human epidermal growth factor receptor; HAPs: hypoxia-activated
prodrugs
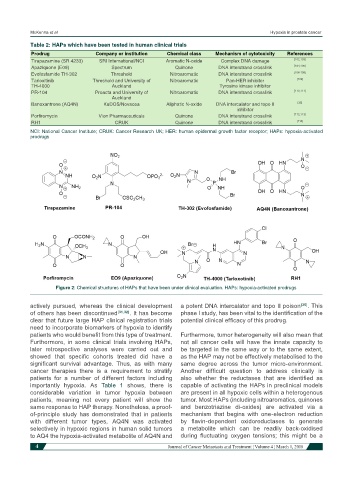
Figure 2: Chemical structures of HAPs that have been under clinical evaluation. HAPs: hypoxia-activated prodrugs
actively pursued, whereas the clinical development a potent DNA intercalator and topo II poison [35] . This
of others has been discontinued [31,32] . It has become phase I study, has been vital to the identification of the
clear that future large HAP clinical registration trials potential clinical efficacy of this prodrug.
need to incorporate biomarkers of hypoxia to identify
patients who would benefit from this type of treatment. Furthermore, tumor heterogeneity will also mean that
Furthermore, in some clinical trials involving HAPs, not all cancer cells will have the innate capacity to
later retrospective analyses were carried out and be targeted in the same way or to the same extent,
showed that specific cohorts treated did have a as the HAP may not be effectively metabolised to the
significant survival advantage. Thus, as with many same degree across the tumor micro-environment.
cancer therapies there is a requirement to stratify Another difficult question to address clinically is
patients for a number of different factors including also whether the reductases that are identified as
importantly hypoxia. As Table 1 shows, there is capable of activating the HAPs in preclinical models
considerable variation in tumor hypoxia between are present in all hypoxic cells within a heterogenous
patients, meaning not every patient will show the tumor. Most HAPs (including nitroaromatics, quinones
same response to HAP therapy. Nonetheless, a proof- and benzotriazine di-oxides) are activated via a
of-principle study has demonstrated that in patients mechanism that begins with one-electron reduction
with different tumor types, AQ4N was activated by flavin-dependent oxidoreductases to generate
selectively in hypoxic regions in human solid tumors a metabolite which can be readily back-oxidised
to AQ4 the hypoxia-activated metabolite of AQ4N and during fluctuating oxygen tensions; this might be a
4 Journal of Cancer Metastasis and Treatment ¦ Volume 4 ¦ March 1, 2018