
Page 125 - Read Online
P. 125
Priya et al. J Cancer Metastasis Treat 2021;7:70 https://dx.doi.org/10.20517/2394-4722.2021.122 Page 9 of 17
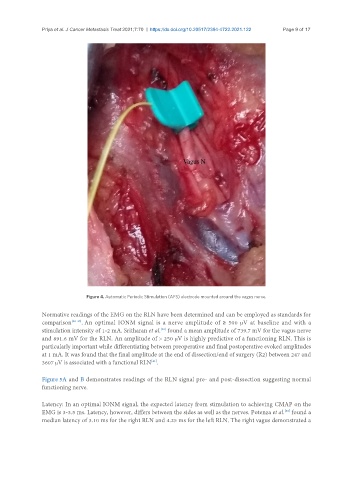
Figure 4. Automatic Periodic Stimulation (APS) electrode mounted around the vagus nerve.
Normative readings of the EMG on the RLN have been determined and can be employed as standards for
comparison [38-40] . An optimal IONM signal is a nerve amplitude of ≥ 500 μV at baseline and with a
[40]
stimulation intensity of 1-2 mA. Sritharan et al. found a mean amplitude of 739.7 mV for the vagus nerve
and 891.6 mV for the RLN. An amplitude of > 250 μV is highly predictive of a functioning RLN. This is
particularly important while differentiating between preoperative and final postoperative evoked amplitudes
at 1 mA. It was found that the final amplitude at the end of dissection/end of surgery (R2) between 247 and
3607 μV is associated with a functional RLN .
[41]
Figure 5A and B demonstrates readings of the RLN signal pre- and post-dissection suggesting normal
functioning nerve.
Latency: In an optimal IONM signal, the expected latency from stimulation to achieving CMAP on the
EMG is 3-3.5 ms. Latency, however, differs between the sides as well as the nerves. Potenza et al. found a
[38]
median latency of 3.10 ms for the right RLN and 4.25 ms for the left RLN. The right vagus demonstrated a