
Page 49 - Read Online
P. 49
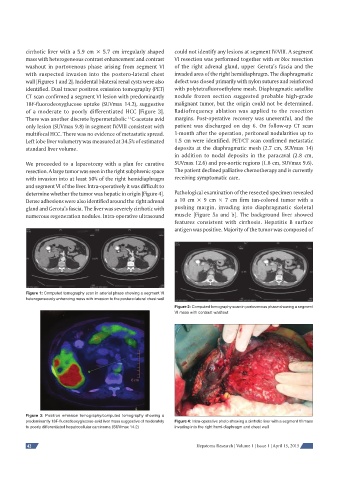
cirrhotic liver with a 5.9 cm × 5.7 cm irregularly shaped could not identify any lesions at segment IV/VIII. A segment
mass with heterogeneous contrast enhancement and contrast VI resection was performed together with en bloc resection
washout in portovenous phase arising from segment VI of the right adrenal gland, upper Gerota’s fascia and the
with suspected invasion into the postero-lateral chest invaded area of the right hemidiaphragm. The diaphragmatic
wall [Figures 1 and 2]. Incidental bilateral renal cysts were also defect was closed primarily with nylon sutures and reinforced
identified. Dual tracer positron emission tomography (PET) with polytetrafluoroethylene mesh. Diaphragmatic satellite
CT scan confirmed a segment VI lesion with predominantly nodule frozen section suggested probable high-grade
18F-fluorodeoxyglucose uptake (SUVmax 14.2), suggestive malignant tumor, but the origin could not be determined.
of a moderate to poorly differentiated HCC [Figure 3]. Radiofrequency ablation was applied to the resection
11
There was another discrete hypermetabolic C-acetate avid margins. Post-operative recovery was uneventful, and the
only lesion (SUVmax 9.8) in segment IV/VIII consistent with patient was discharged on day 6. On follow-up CT scan
multifocal HCC. There was no evidence of metastatic spread. 1-month after the operation, peritoneal nodularities up to
Left lobe liver volumetry was measured at 34.5% of estimated 1.5 cm were identified. PET/CT scan confirmed metastatic
standard liver volume. deposits at the diaphragmatic mesh (2.7 cm, SUVmax 14)
in addition to nodal deposits in the paracaval (2.8 cm,
We proceeded to a laparotomy with a plan for curative SUVmax 12.6) and pre-aortic regions (1.8 cm, SUVmax 9.6).
resection. A large tumor was seen in the right subphrenic space The patient declined palliative chemotherapy and is currently
with invasion into at least 50% of the right hemidiaphragm receiving symptomatic care.
and segment VI of the liver. Intra-operatively it was difficult to
determine whether the tumor was hepatic in origin [Figure 4]. Pathological examination of the resected specimen revealed
Dense adhesions were also identified around the right adrenal a 10 cm × 9 cm × 7 cm firm tan-colored tumor with a
gland and Gerota’s fascia. The liver was severely cirrhotic with pushing margin, invading into diaphragmatic skeletal
numerous regeneration nodules. Intra-operative ultrasound muscle [Figure 5a and b]. The background liver showed
features consistent with cirrhosis. Hepatitis B surface
antigen was positive. Majority of the tumor was composed of
Figure 1: Computed tomography scan in arterial phase showing a segment VI
heterogeneously enhancing mass with invasion to the postero-lateral chest wall
Figure 2: Computed tomography scan in portovenous phase showing a segment
VI mass with contrast washout
Figure 3: Positron emission tomography/computed tomography showing a
predominantly 18F-fl uorodeoxyglucose-avid liver mass suggestive of moderately Figure 4: Intra-operative photo showing a cirrhotic liver with a segment VI mass
to poorly differentiated hepatocellular carcinoma (SUVmax 14.2) invading into the right hemi-diaphragm and chest wall
42 Hepatoma Research | Volume 1 | Issue 1 | April 15, 2015