
Page 44 - Read Online
P. 44
METHODS Statistical analysis
Chi-square test and Fisher’s t-test whenever appropriate
Patients selection were used for categorical variables and Mann-Whitney U-test
All the patients transplanted for hepatitis C related liver for continues variables. Kaplan-Meier survival curves were
disease with HCC were analyzed retrospectively. All the data prepared for recurrences and mortality with the Log-rank
collected was at the time of liver transplant. Barcelona clinic test. Multivariate analysis was performed using multivariate
liver cancer staging criteria were followed to decide treatment Cox regression analysis. SPSS version 21 (IBM, Armonk, NY,
options. University of California, San Fransisco (UCSF) USA) was used for statistical analysis. Two-tailed significances
criteria were used as transplantation indication. If the were taken into consideration. P < 0.05 was considered as
[7]
tumor was outside UCSF criteria, loco-regional therapies statistically significant.
such as transarterial chemoembolization, radiofrequency
ablation were used. These patients were scheduled for RESULTS
transplantation when they fulfilled UCSF criteria. Results
with down staging are published before. Patients who One hundred and nine patients underwent living donor LT
[8]
underwent liver resections before and subsequently for HCV-related HCC between July 2002 and November 2012.
transplanted for intrahepatic recurrence were included in Median follow-up time was 31 months. Eighteen patients
salvage transplant group, and other patients who were underwent salvage transplantation for intrahepatic recurrence
transplanted without prior resection were included in the post-hepatectomy; while 91 patients underwent primary
primary transplant group. The review board of Chang Gung transplants. Patients’ characteristics are described in Table 1.
Memorial Hospital approved this study.
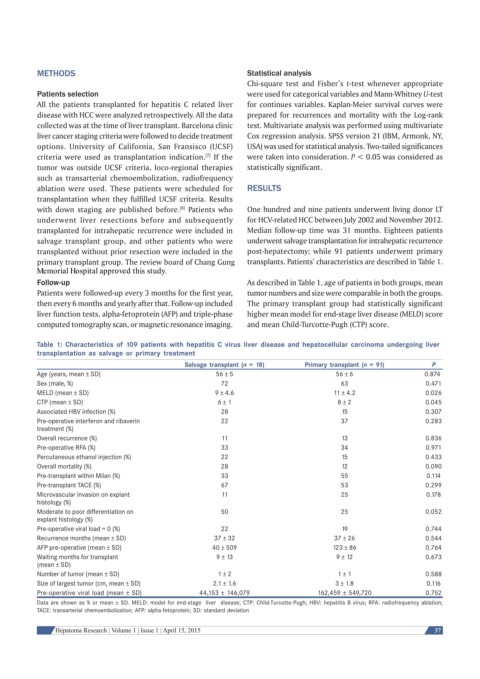
Follow-up As described in Table 1, age of patients in both groups, mean
Patients were followed-up every 3 months for the first year, tumor numbers and size were comparable in both the groups.
then every 6 months and yearly after that. Follow-up included The primary transplant group had statistically significant
liver function tests, alpha-fetoprotein (AFP) and triple-phase higher mean model for end-stage liver disease (MELD) score
computed tomography scan, or magnetic resonance imaging. and mean Child-Turcotte-Pugh (CTP) score.
Table 1: Characteristics of 109 patients with hepatitis C virus liver disease and hepatocellular carcinoma undergoing liver
transplantation as salvage or primary treatment
Salvage transplant (n = 18) Primary transplant (n = 91) P
Age (years, mean ± SD) 56 ± 5 56 ± 6 0.874
Sex (male, %) 72 63 0.471
MELD (mean ± SD) 9 ± 4.6 11 ± 4.2 0.026
CTP (mean ± SD) 6 ± 1 8 ± 2 0.045
Associated HBV infection (%) 28 15 0.307
Pre-operative interferon and ribaverin 22 37 0.283
treatment (%)
Overall recurrence (%) 11 13 0.836
Pre-operative RFA (%) 33 34 0.971
Percutaneous ethanol injection (%) 22 15 0.433
Overall mortality (%) 28 12 0.090
Pre-transplant within Milan (%) 33 55 0.114
Pre-transplant TACE (%) 67 53 0.299
Microvascular invasion on explant 11 25 0.178
histology (%)
Moderate to poor differentiation on 50 25 0.052
explant histology (%)
Pre-operative viral load = 0 (%) 22 19 0.744
Recurrence months (mean ± SD) 37 ± 32 37 ± 26 0.544
AFP pre-operative (mean ± SD) 40 ± 509 123 ± 86 0.764
Waiting months for transplant 9 ± 13 9 ± 12 0.673
(mean ± SD)
Number of tumor (mean ± SD) 1 ± 2 1 ± 1 0.588
Size of largest tumor (cm, mean ± SD) 2.1 ± 1.6 3 ± 1.8 0.116
Pre-operative viral load (mean ± SD) 44,153 ± 146,079 162,459 ± 549,720 0.752
Data are shown as % or mean ± SD. MELD: model for end-stage liver disease; CTP: Child-Turcotte-Pugh; HBV: hepatitis B virus; RFA: radiofrequency ablation;
TACE: transarterial chemoembolization; AFP: alpha-fetoprotein; SD: standard deviation
Hepatoma Research | Volume 1 | Issue 1 | April 15, 2015 37