
Page 74 - Read Online
P. 74
Calinescu et al. Hepatoma Res 2021;7:59 https://dx.doi.org/10.20517/2394-5079.2021.26 Page 9 of 17
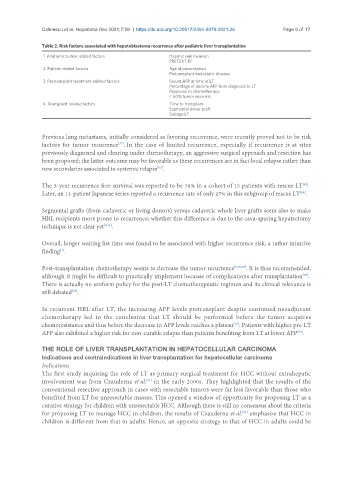
Table 2. Risk factors associated with hepatoblastoma recurrence after pediatric liver transplantation
1. Anatomic tumor related factors Hepatic vein invasion
PRETEXT IV
2. Patient related factors Age at presentation
Pretransplant metastatic disease
3. Pretransplant treatment related factors Serum AFP at time of LT
Percentage of decline AFP from diagnosis to LT
Response to chemotherapy
< 50% tumor necrosis
4. Transplant related factors Time to transplant
Segmental donor graft
Salvage LT
Previous lung metastases, initially considered as favoring recurrence, were recently proved not to be risk
factors for tumor recurrence . In the case of limited recurrence, especially if recurrence is at sites
[77]
previously diagnosed and clearing under chemotherapy, an aggressive surgical approach and resection has
been proposed; the latter outcome may be favorable as these recurrences are in fact local relapse rather than
new secondaries associated to systemic relapse .
[62]
The 3-year recurrence free survival was reported to be 78% in a cohort of 15 patients with rescue LT .
[62]
Later, an 11-patient Japanese series reported a recurrence rate of only 27% in this subgroup of rescue LT .
[68]
Segmental grafts (from cadaveric or living donors) versus cadaveric whole liver grafts seem also to make
HBL recipients more prone to recurrence; whether this difference is due to the cava-sparing hepatectomy
technique is not clear yet [8,11] .
Overall, longer waiting list time was found to be associated with higher recurrence risk, a rather intuitive
[4]
finding .
Post-transplantation chemotherapy seems to decrease the tumor recurrence [6,73,78] . It is thus recommended,
although it might be difficult to practically implement because of complications after transplantation .
[73]
There is actually no uniform policy for the post-LT chemotherapeutic regimen and its clinical relevance is
still debated .
[68]
In recurrent HBL after LT, the increasing AFP levels pretransplant despite continued neoadjuvant
chemotherapy led to the conclusion that LT should be performed before the tumor acquires
chemoresistance and thus before the decrease in AFP levels reaches a plateau . Patients with higher pre-LT
[79]
AFP also exhibited a higher risk for non-curable relapse than patients benefiting from LT at lower AFP .
[80]
THE ROLE OF LIVER TRANSPLANTATION IN HEPATOCELLULAR CARCINOMA
Indications and contraindications in liver transplantation for hepatocellular carcinoma
Indications
The first study inquiring the role of LT as primary surgical treatment for HCC without extrahepatic
involvement was from Czauderna et al. in the early 2000s. They highlighted that the results of the
[81]
conventional resective approach in cases with resectable tumors were far less favorable than those who
benefited from LT for unresectable masses. This opened a window of opportunity for proposing LT as a
curative strategy for children with unresectable HCC. Although there is still no consensus about the criteria
for proposing LT to manage HCC in children, the results of Czauderna et al. emphasize that HCC in
[81]
children is different from that in adults. Hence, an opposite strategy to that of HCC in adults could be