
Page 64 - Read Online
P. 64
Kato et al. Hepatoma Res 2021;7:10 I http://dx.doi.org/10.20517/2394-5079.2020.129 Page 5 of 15
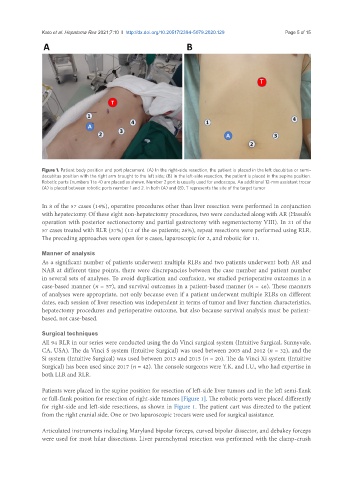
Figure 1. Patient body position and port placement. (A) In the right-side resection, the patient is placed in the left decubitus or semi-
decubitus position with the right arm brought to the left side; (B) in the left-side resection, the patient is placed in the supine position.
Robotic ports (numbers 1 to 4) are placed as shown. Number 2 port is usually used for endoscope. An additional 12-mm assistant trocar
(A) is placed between robotic ports number 1 and 2. In both (A) and (B), T represents the site of the target tumor
In 8 of the 57 cases (14%), operative procedures other than liver resection were performed in conjunction
with hepatectomy. Of these eight non-hepatectomy procedures, two were conducted along with AR (Hassab’s
operation with posterior sectionectomy and partial gastrectomy with segmentectomy VIII). In 21 of the
57 cases treated with RLR (37%) (12 of the 46 patients; 26%), repeat resections were performed using RLR.
The preceding approaches were open for 8 cases, laparoscopic for 2, and robotic for 11.
Manner of analysis
As a significant number of patients underwent multiple RLRs and two patients underwent both AR and
NAR at different time points, there were discrepancies between the case number and patient number
in several sets of analyses. To avoid duplication and confusion, we studied perioperative outcomes in a
case-based manner (n = 57), and survival outcomes in a patient-based manner (n = 46). These manners
of analyses were appropriate, not only because even if a patient underwent multiple RLRs on different
dates, each session of liver resection was independent in terms of tumor and liver function characteristics,
hepatectomy procedures and perioperative outcome, but also because survival analysis must be patient-
based, not case-based.
Surgical techniques
All 94 RLR in our series were conducted using the da Vinci surgical system (Intuitive Surgical, Sunnyvale,
CA, USA). The da Vinci S system (Intuitive Surgical) was used between 2005 and 2012 (n = 32), and the
Si system (Intuitive Surgical) was used between 2013 and 2015 (n = 20). The da Vinci Xi system (Intuitive
Surgical) has been used since 2017 (n = 42). The console surgeons were Y.K. and I.U., who had expertise in
both LLR and RLR.
Patients were placed in the supine position for resection of left-side liver tumors and in the left semi-flank
or full-flank position for resection of right-side tumors [Figure 1]. The robotic ports were placed differently
for right-side and left-side resections, as shown in Figure 1. The patient cart was directed to the patient
from the right cranial side. One or two laparoscopic trocars were used for surgical assistance.
Articulated instruments including Maryland bipolar forceps, curved bipolar dissector, and debakey forceps
were used for most hilar dissections. Liver parenchymal resection was performed with the clamp-crush