
Page 348 - Read Online
P. 348
Spieker et al. Vessel Plus 2020;4:29 I http://dx.doi.org/10.20517/2574-1209.2020.28 Page 7 of 11
n
n n
n
n
n
n
n n
n
n n
n
n
n
n
n n
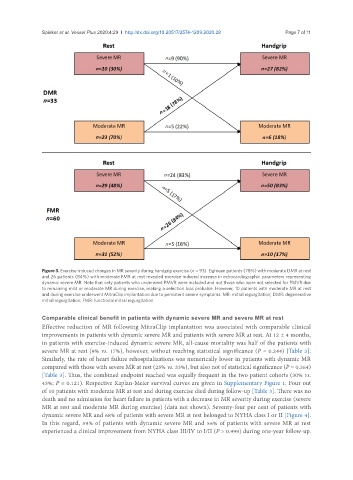
Figure 3. Exercise-induced changes in MR severity during handgrip exercise (n = 93). Eighteen patients (78%) with moderate DMR at rest
and 26 patients (84%) with moderate FMR at rest revealed exercise-induced increase in echocardiographic parameters representing
dynamic severe MR. Note that only patients who underwent PMVR were included and not those who were not selected for PMVR due
to remaining mild or moderate MR during exercise, making a selection bias probable. However, 10 patients with moderate MR at rest
and during exercise underwent MitraClip implantation due to persistent severe symptoms. MR: mitral regurgitation; DMR: degenerative
mitral regurgitation; FMR: functional mitral regurgitation
Comparable clinical benefit in patients with dynamic severe MR and severe MR at rest
Effective reduction of MR following MitraClip implantation was associated with comparable clinical
improvements in patients with dynamic severe MR and patients with severe MR at rest. At 12 ± 4 months,
in patients with exercise-induced dynamic severe MR, all-cause mortality was half of the patients with
severe MR at rest (9% vs. 17%), however, without reaching statistical significance (P = 0.244) [Table 3].
Similarly, the rate of heart failure rehospitalizations was numerically lower in patients with dynamic MR
compared with those with severe MR at rest (25% vs. 33%), but also not of statistical significance (P = 0.364)
[Table 3]. Thus, the combined endpoint reached was equally frequent in the two patient cohorts (30% vs.
43%; P = 0.121). Respective Kaplan-Meier survival curves are given in Supplementary Figure 1. Four out
of 10 patients with moderate MR at rest and during exercise died during follow-up [Table 3]. There was no
death and no admission for heart failure in patients with a decrease in MR severity during exercise (severe
MR at rest and moderate MR during exercise) (data not shown). Seventy-four per cent of patients with
dynamic severe MR and 68% of patients with severe MR at rest belonged to NYHA class I or II [Figure 4].
In this regard, 59% of patients with dynamic severe MR and 56% of patients with severe MR at rest
experienced a clinical improvement from NYHA class III/IV to I/II (P > 0.999) during one-year follow-up.