
Page 60 - Read Online
P. 60
Page 6 of 21 Dokko et al. Vessel Plus 2022;6:37 https://dx.doi.org/10.20517/2574-1209.2021.121
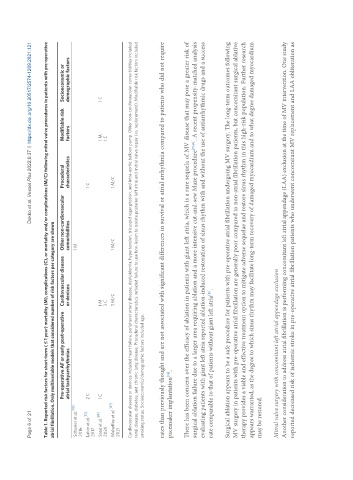
Table 1. Reported risk factors for short-term ( ≤ 1 year) mortality (M), complications (C), or mortality and/or complications (M/C) following mitral valve procedures in patients with pre-operative
atrial fibrillation. Only multivariable models that considered number of risk factors per category are shown
Pre-operative AF or early post-operative Cardiovascular disease Other non-cardiovascular Procedural Modifiable risk Socioeconomic or
atrial tachyarrhythmias or devices comorbidities characteristics factors demographic factors
[140]
Schueler et al. 1 M
2016
[57]
Labin et al. 2 C 1 C
2017
Saad et al. [89] 1 C 1 M 1 M 1 C
2020 3 C 1 C
Mehaffey et al. [137] 3 M/C 1 M/C 1 M/C
2021
Cardiovascular disease or devices included heart failure, peripheral artery disease, dyslipidemia, hypertension, tricuspid regurgitation, and intra-aortic balloon pump. Other non-cardiovascular comorbidities included
renal disease, diabetes, and chronic lung disease. Procedural characteristics included failure to use box-lesion to isolate posterior left atria and mitral valve repair (vs. replacement). Modifiable risk factors included
smoking status. Socioeconomic/demographic factors included age.
rates than previously thought and are not associated with significant differences in survival or atrial arrhythmia compared to patients who did not require
pacemaker implantation .
[78]
There has been concern over the efficacy of ablation in patients with giant left atria, which is a rare sequela of MV disease that may pose a greater risk of
surgical ablation failure due to a larger area requiring ablation and a more intensive cut-and-sew Maze procedure [79,80] . A recent propensity-matched analysis
evaluating patients with giant left atria reported ablation-induced restoration of sinus rhythm with and without the use of antiarrhythmic drugs and a success
rate comparable to that of patients without giant left atria .
[80]
Surgical ablation appears to be a safe procedure for patients with pre-operative atrial fibrillation undergoing MV surgery. The long-term outcomes following
MV surgery in patients with pre-operative atrial fibrillation are generally poor compared to non-atrial fibrillation patients, but concomitant surgical ablative
therapy provides a viable and effective treatment option to mitigate adverse sequelae and restore sinus rhythm in this high-risk population. Further research
appears warranted, as the degree to which sinus rhythm may facilitate long-term recovery of damaged myocardium and to what degree damaged myocardium
may be restored.
Mitral valve surgery with concomitant left atrial appendage exclusion
Another consideration to address atrial fibrillation is performing concomitant left atrial appendage (LAA) exclusion at the time of MV intervention. One study
reported decreased risk of ischemic stroke in pre-operative atrial fibrillation patients who underwent concomitant MV replacement and LAA obliteration as