
Page 287 - Read Online
P. 287
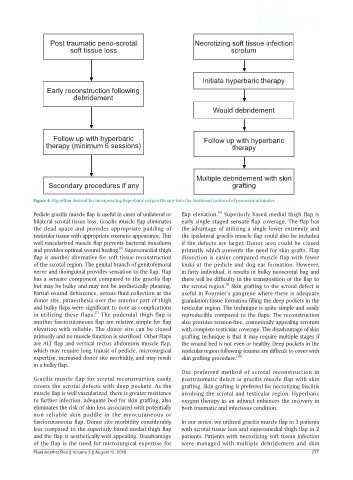
Post traumatic peno-scrotal Necrotizing soft tissue infection
soft tissue loss scrotum
Initiate hyperbaric therapy
Early reconstruction following
debridement
Would debridement
Follow up with hyperbaric Follow up with hyperbaric
therapy (minimum 6 sessions) therapy
Multiple debridement with skin
Secondary procedures if any grafting
Figure 4: Algorithm devised for incorporating hyperbaric oxygen therapy into the treatment protocol of penoscrotal injuries
[8]
Pedicle gracilis muscle flap is useful in cases of unilateral or flap elevation. Superiorly based medial thigh flap is
bilateral scrotal tissue loss. Gracilis muscle flap eliminates early single staged sensate flap coverage. The flap has
the dead space and provides appropriate padding of the advantage of utilizing a single lower extremity and
testicular tissue with appropriate cosmetic appearance. This the ipsilateral gracilis muscle flap could also be included
well vascularized muscle flap prevents bacterial inoculums if the defects are larger. Donor area could be closed
[6]
and provides optimal wound healing. Superomedial thigh primarily which prevents the need for skin grafts. Flap
flap is another alternative for soft tissue reconstruction dissection is easier compared muscle flap with fewer
of the scrotal region. The genital branch of genitofemoral kinks at the pedicle and dog ear formation. However,
nerve and ilioinguinal provides sensation to the flap. Flap in fatty individual, it results in bulky neoscrotal bag and
has a sensate component compared to the gracilis flap there will be difficulty in the transposition of the flap to
but may be bulky and may not be aesthetically pleasing. the scrotal region. Skin grafting to the scrotal defect is
[9]
Partial wound dehiscence, serous fluid collection at the useful in Fournier’s gangrene where there is adequate
donor site, paraesthesia over the anterior part of thigh granulation tissue formation filling the deep pockets in the
and bulky flaps were significant to note as complications testicular region. The technique is quite simple and easily
in utilizing these flaps. The pudendal thigh flap is reproducible compared to the flaps. The reconstruction
[7]
another fasciocutaneous flap are relative simple for flap also provides tension-free, cosmetically appealing scrotum
elevation with reliable. The donor site can be closed with complete testicular coverage. The disadvantage of skin
primarily and no muscle function is sacrificed. Other Flaps grafting technique is that it may require multiple stages if
are ALT flap and vertical rectus abdominis muscle flap, the wound bed is not even or healthy. Deep pockets in the
which may require long transit of pedicle, microsurgical testicular region following trauma are difficult to cover with
expertise, increased donor site morbidity, and may result skin grafting procedure. [10]
in a bulky flap.
Our preferred method of scrotal reconstruction in
Gracilis muscle flap for scrotal reconstruction easily posttraumatic defect is gracilis muscle flap with skin
covers the scrotal defects with deep pockets. As the grafting. Skin grafting is preferred for necrotizing fasciitis
muscle flap is well vascularized, there is greater resistance involving the scrotal and testicular region. Hyperbaric
to further infection, adequate bed for skin grafting, also oxygen therapy as an adjunct enhances the recovery in
eliminates the risk of skin loss associated with potentially both traumatic and infectious condition.
non reliable skin paddle in the myocutaneous or
fasciocutaneous flap. Donor site morbidity considerably In our series, we utilized gracilis muscle flap in 3 patients
less compared to the superiorly based medial thigh flap with scrotal tissue loss and superomedial thigh flap in 2
and the flap is aesthetically well appealing. Disadvantage patients. Patients with necrotizing soft tissue infection
of the flap is the need for microsurgical expertise for were managed with multiple debridement and skin
Plast Aesthet Res || Volume 3 || August 12, 2016 277