
Page 9 - Read Online
P. 9
Page 4 of 17 Buncke. Plast Aesthet Res 2022;9:38 https://dx.doi.org/10.20517/2347-9264.2022.08
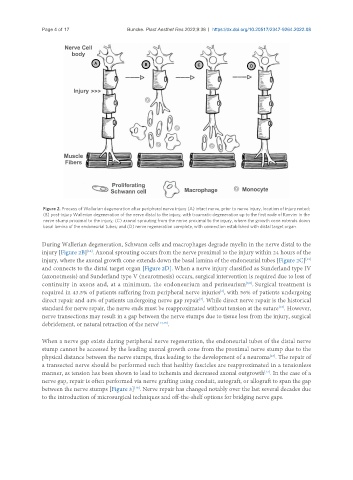
Figure 2. Process of Wallerian degeneration after peripheral nerve injury (A) intact nerve, prior to nerve injury, location of injury noted;
(B) post-injury Wallerian degeneration of the nerve distal to the injury, with traumatic degeneration up to the first node of Ranvier in the
nerve stump proximal to the injury; (C) axonal sprouting from the nerve proximal to the injury, where the growth cone extends down
basal lamina of the endoneurial tubes; and (D) nerve regeneration complete, with connection established with distal target organ.
During Wallerian degeneration, Schwann cells and macrophages degrade myelin in the nerve distal to the
injury [Figure 2B] . Axonal sprouting occurs from the nerve proximal to the injury within 24 hours of the
[12]
injury, where the axonal growth cone extends down the basal lamina of the endoneurial tubes [Figure 2C]
[11]
and connects to the distal target organ [Figure 2D]. When a nerve injury classified as Sunderland type IV
(axonotmesis) and Sunderland type V (neurotmesis) occurs, surgical intervention is required due to loss of
continuity in axons and, at a minimum, the endoneurium and perineurium . Surgical treatment is
[8,9]
required in 43.5% of patients suffering from peripheral nerve injuries , with 56% of patients undergoing
[2]
direct repair and 44% of patients undergoing nerve gap repair . While direct nerve repair is the historical
[3]
standard for nerve repair, the nerve ends must be reapproximated without tension at the suture . However,
[13]
nerve transections may result in a gap between the nerve stumps due to tissue loss from the injury, surgical
debridement, or natural retraction of the nerve [14,15] .
When a nerve gap exists during peripheral nerve regeneration, the endoneurial tubes of the distal nerve
stump cannot be accessed by the leading axonal growth cone from the proximal nerve stump due to the
physical distance between the nerve stumps, thus leading to the development of a neuroma . The repair of
[16]
a transected nerve should be performed such that healthy fascicles are reapproximated in a tensionless
manner, as tension has been shown to lead to ischemia and decreased axonal outgrowth . In the case of a
[17]
nerve gap, repair is often performed via nerve grafting using conduit, autograft, or allograft to span the gap
between the nerve stumps [Figure 3] . Nerve repair has changed notably over the last several decades due
[18]
to the introduction of microsurgical techniques and off-the-shelf options for bridging nerve gaps.