
Page 68 - Read Online
P. 68
Oliver et al. Plast Aesthet Res. 2025;12:19 https://dx.doi.org/10.20517/2347-9264.2025.11 Page 9 of 16
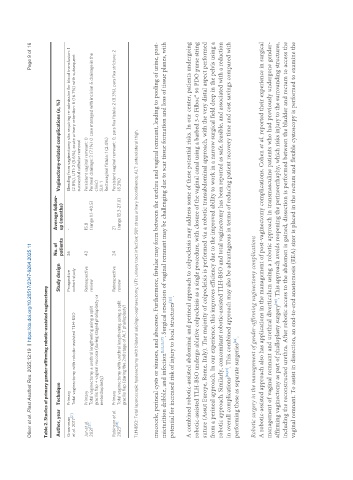
Table 2. Studies of primary gender-affirming robotic-assisted vaginectomy
No. of Average follow-
Author, year Technique Study design Vaginectomy-related complications (n, %)
patients up (months)
Groenman Primary Prospective 36 - Bleeding from vaginectomy site requiring re-admission for blood transfusion: 1
et al. 2017 [21] Total vaginectomy with robotic-assisted TLH-BSO cohort study (2.8%), UTI: 2 (5.6%), acute urinary retention: 6 (16.7%) with subsequent
successful catheter removal
Jun et al. Primary Retrospective 42 15.8 Persistent vaginal remnant: 0
[27]
2021 Total vaginectomy ± urethral lengthening using a split review (range 1.1-40.5) Perineal drainage: 3 (7.1%) (1 case managed with incision & drainage in the
gracilis flap + vaginal mucosa (during staged phalloplasty or clinic)
metoidioplasty) SUI: 1
Rectovaginal fistula: 1 (2.4%)
Robinson et al. Primary Retrospective 24 21 Persistent vaginal remnant: 0, pars fixa fistula: 2 (8.3%), pars fixa stricture: 2
[25]
2023 Total vaginectomy with urethral lengthening using a split review (range 13.3-27.0) (8.3%)
gracilis flap (during the 2nd stage of ALT phalloplasty)
TLH-BSO: Total laparoscopic hysterectomy with bilateral salpingo-oophorectomy; UTI: urinary tract infection; SUI: stress urinary incontinence; ALT: anterolateral thigh.
mucocele, perineal cysts or sinuses, and abscesses. Furthermore, fistulae may form between the urethra and vaginal remnant, leading to pooling of urine, post-
micturition dribble, and infection [3,22,23,27] . Surgical resection of vaginal remnant may be challenging due to scar tissue formation and loss of tissue planes, with
potential for increased risk of injury to local structures .
[22]
A combined robotic-assisted abdominal and perineal approach to colpocleisis may address some of these potential risks. In our center, patients undergoing
robotic-assisted TLH-BSO undergo ablative colpocleisis as a single procedure, with closure of the vaginal canal using a barbed 3-0 Filboc® 90 PDO purse string
suture (Assut Europe, Rome, Italy). The majority of colpocleisis is performed via a robotic transabdominal approach, with the very distal aspect performed
from a perineal approach. In our experience, this improves efficiency due to the improved ability to work in a narrow surgical field deep in the pelvis using a
robotic approach. Similarly, concomitant robotic-assisted TLH-BSO and total vaginectomy has been reported as safe, feasible, and associated with a reduction
in overall complications [23,27] . This combined approach may also be advantageous in terms of reducing patient recovery time and cost savings compared with
performing these as separate surgeries .
[28]
Robotic surgery in the management of gender-affirming vaginectomy complications
A robotic-assisted approach also has applications in the management of post-vaginectomy complications. Cohen et al. reported their experience in surgical
management of vaginal remnant and urethral diverticulum using a robotic approach in transmasculine patients who had previously undergone gender-
affirming vaginectomy as part of phalloplasty surgery . This approach avoids reopening the perineorrhaphy, which risks injury to the surrounding structures,
[30]
including the reconstructed urethra. After robotic access to the abdomen is gained, dissection is performed between the bladder and rectum to access the
vaginal remnant. To assist in dissection, an end-to-end anastomosis (EEA) sizer is placed in the rectum and flexible cystoscopy is performed to examine the