
Page 70 - Read Online
P. 70
Oliver et al. Plast Aesthet Res. 2025;12:19 https://dx.doi.org/10.20517/2347-9264.2025.11 Page 11 of 16
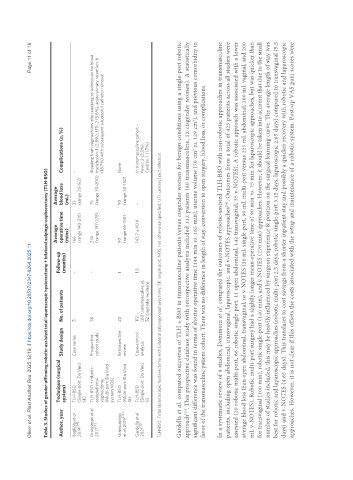
Table 3. Studies of gender-affirming robotic-assisted total laparoscopic hysterectomy + bilateral salpingo-oophorectomy (TLH-BSO)
Average Average
Technique (surgical Follow-up
Author, year Study design No. of patients operative time blood loss Complications (n, %)
system) (months) (mins) (mL)
Bogliolo et al. TLH-BSO Case series 5 - 166 33 -
[34]
2014 (Single-port: Da Vinci (range 140-210) (range 20-50)
SP)
Groenman et al. TLH-BSO + robotic- Prospective 36 - 230 75 Bleeding from vaginectomy site requiring re-admission for blood
2017 [21] assisted total cohort study (range 197-278) (range 30-200) transfusion: 1 (2.8%), UTI: 2 (5.6%), acute urinary retention: 6
vaginectomy (16.7%) with subsequent successful catheter removal
(Multi-port: Da Vinci
system NOS)
Giampaolino TLH-BSO Retrospective 20 1 90 90 None
et al. 2019 [33] (Multi-port: Da Vinci review (range 65-150) (range 30-150)
Xi)
Gardella et al. TLH-BSO Case-control 112 1.5 143.7 ± 40.4 - In transmasculine cohort -
[35]
2021 (Single-port: Da Vinci analysis (60 transmasculine vs. Fever: 2 (3.3%),
Si) 52 cisgender women) Cystitis: 1 (1.7%)
TLH-BSO: Total laparoscopic hysterectomy with bilateral salpingo-oophorectomy; SP: single port; NOS: not otherwise specified; UTI: urinary tract infection.
Gardella et al. compared outcomes of TLH ± BSO in transmasculine patients versus cisgender women for benign conditions using a single-port robotic
[35]
approach . This prospective database study with retrospective analysis included 112 patients (60 transmasculine, 52 cisgender women). A statistically
significant difference was found in terms of shorter operative time (144 min vs. 165 min), uterine volume (70 cm vs. 129 cm ), and previous comorbidity in
3
3
favor of the transmasculine patient cohort. There was no difference in length of stay, conversion to open surgery, blood loss, or complications.
In a systematic review of 8 studies, Dominoni et al. compared the outcomes of robotic-assisted TLH-BSO with non-robotic approaches in transmasculine
[36]
patients, including open abdominal, transvaginal, laparoscopic, and v-NOTES approaches . Outcomes from a total of 425 patients across all studies were
assessed (20 robotic multi-port, 66 robotic single-port, 11 open abdominal, 142 transvaginal, 35 v-NOTES). A robotic approach was associated with a lower
average blood loss than open abdominal, transvaginal, or v-NOTES (30 mL single-port, 90 mL multi-port versus 225 mL abdominal, 200 mL vaginal, and 200
mL v-NOTES). Robotic multi-port surgery had a slightly longer mean operative time of 90 min vs. 75 min for laparoscopic approaches, but was quicker than
for transvaginal (100 min), robotic single-port (140 min), and v-NOTES (270 min) approaches. However, it should be taken into account that due to the small
number of studies included, this may be heavily influenced by surgeon experience & position on the surgical learning curve. The average length of stay was
best for robotic and laparoscopic approaches (robotic multi-port 2.5 days, robotic single-port 3.15 days, laparoscopic 2.65 days) compared to transvaginal (5.5
days) and v-NOTES (4.65 days). This translates to cost savings from a shorter inpatient stay and possibly a quicker recovery with robotic and laparoscopic
approaches. However, it is not clear if this offsets the costs associated with the setup and maintenance of a robotic system. Post-op VAS pain scores were