
Page 63 - Read Online
P. 63
Page 4 of 16 Oliver et al. Plast Aesthet Res. 2025;12:19 https://dx.doi.org/10.20517/2347-9264.2025.11
revision - peritoneal
flap)
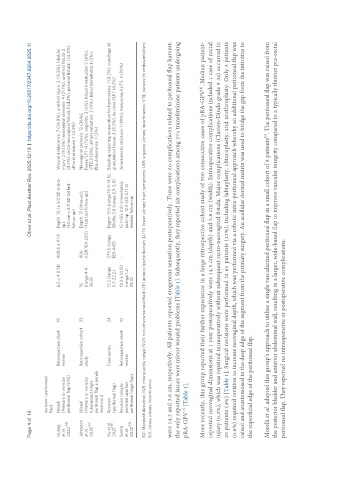
Huang Mixed Retrospective chart 19 6.5 ± 4.0 SD 408.6 ± 111.9 Depth: 13.1 ± 3.0 SD (intra- Wound dehiscence: 7 (36.8%), urethral injury: 3 (15.8%), bladder
et al. (Primary or revision review op), injury: 2 (10.5%) neovaginal stenosis: 4 (21.1%), urethral fistula: 2
[16]
2022 peritoneal flap NOS) 11.0 cm ± 4.0 SD (at last (8.7%), recto-neovaginal fistula: 1 (4.3%), perianal fistula: 1 (4.3%),
follow-up) clitoral prolapse: 1 (4.3%)
Johnston Mixed Retrospective cohort 33 16 406 Depth: 17 (intra-op), Neovaginal stenosis: 12 (36%),
et al. (Primary or revision study (range 4.4- (IQR 154-220) 11 (at last follow-up) Fever/UTI: 4 (12%), vaginitis: 2 (6%), blood transfusion: 2 (6%),
[10]
2025 tubularized single 26.9) VTE: 1 (3%), urinary retention: 3 (9%), labial hematoma: 1 (3%),
peritoneal flap ± penile flap dehiscence: 1 (3%)
inversion)
Dy et al. Revision Case series 24 13.2 (range 279.5 (range Depth: 13.6 (range 10.9-14.5), Bleeding requiring reoperation for hemostasis: 1 (4.2%), curettage of
2021 [17] (peritoneal flap) 5.7-22.2) 183-443) Width: 3.6 (range 2.9-3.8) granulation tissue: 2 (8.3%), de novo SUI 1 (4.2%)
Smith Revision (single- Retrospective chart 10 18.3 ± 14 SD - 15.1 (SD 2.2) immediately Anastomotic stricture: 1 (10%), temporary LUTS: 3 (30%)
et al. pedicled urachus review (range 1.2- post-op, 12.5 (SD 2.1) at
[18]
2022 peritoneal hinge flap) 39.4) median follow-up
SD: Standard deviation; IQR: interquartile range; NOS: not otherwise specified; UTI: urinary tract infection; LUTS: lower urinary tract symptoms; UUI: urgency urinary incontinence; VTE: venous thromboembolism;
SUI: stress urinary incontinence.
were 14.2 and 3.6 cm, respectively. All patients reported erogenous sensation postoperatively. There were no complications related to peritoneal flap harvest;
the only reported issues were minor wound problems [Table 1]. Subsequently, they reported six complications among 274 transfeminine patients undergoing
pRA-GPV [Table 1].
[7]
[8]
More recently, this group reported their further experience in a large retrospective cohort study of 500 consecutive cases of pRA-GPV . Median patient-
reported neovaginal dimensions at 1 year postoperatively were 14.5 cm (depth) and 3.8 cm (width). Intraoperative complications included 1 case of rectal
injury (0.2%), which was repaired intraoperatively without subsequent recto-neovaginal fistula. Major complications (Clavien-Dindo grade ≥ 3a) occurred in
20 patients (4%) [Table 1]. Surgical revisions were performed in 61 patients (12%), including labiaplasty, clitoroplasty, and urethroplasty. Only 3 patients
(0.6%) required revision to increase neovaginal depth, which was performed via a robotic intra-peritoneal approach whereby an additional peritoneal flap was
raised and anastomosed to the deep edge of the segment from the primary surgery. An acellular dermal matrix was used to bridge the gap from the introitus to
the superficial edge of the peritoneal flap.
[9]
Morelli et al. adapted this group’s approach to utilize a single vascularized peritoneal flap in a small cohort of 8 patients . The peritoneal flap was raised from
the posterior bladder and anterior abdominal wall, resulting in a larger, wide-based flap to improve vascular integrity compared to a typically thinner pre-rectal
peritoneal flap. They reported no intraoperative or postoperative complications.