
Page 134 - Read Online
P. 134
Chao et al. Plast Aesthet Res. 2025;12:29 https://dx.doi.org/10.20517/2347-9264.2025.18 Page 7 of 13
Table 1. Complications of full-depth and revision vaginoplasty with robotic assistance (n = 127)
Complication Full-depth vaginoplasty (%) Revision vaginoplasty (%) Total (%)
No. 99 28 127
Rectal injury 0 (0) 0 (0) 0 (0)
Urethral injury 1 (1.0) 0 (0) 1 (0.8)
Fistula 0 (0) 0 (0) 0 (0)
Transfusion 14 (14.0) 0 (0) 14 (11.0)
Hematoma 1 (1.0) 0 (0) 1 (0.8)
Abscess 2 (2.0) 0 (0) 2 (1.6)
Small bowel obstruction 0 (0) 0 (0) 0 (0)
,
Neovaginal stenosis or loss of depth 7 (7.1) 7 (25.0) 14 (11.0)
Requiring operative intervention; Revision procedures for neovaginal stenosis or loss of depth include intraoperative dilation, scar incision,
Kenalog injection, and/or robotic-assisted revision vaginoplasty.
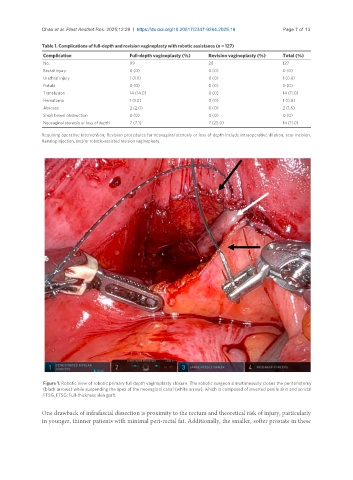
Figure 1. Robotic view of robotic primary full depth vaginoplasty closure. The robotic surgeon simultaneously closes the peritonotomy
(black arrows) while suspending the apex of the neovaginal canal (white arrow), which is composed of inverted penile skin and scrotal
FTSG. FTSG: Full-thickness skin graft.
One drawback of infrafascial dissection is proximity to the rectum and theoretical risk of injury, particularly
in younger, thinner patients with minimal peri-rectal fat. Additionally, the smaller, softer prostate in these