
Page 30 - Read Online
P. 30
Page 12 of 15 Crowe et al. Plast Aesthet Res 2019;6:4 I http://dx.doi.org/10.20517/2347-9264.2018.70
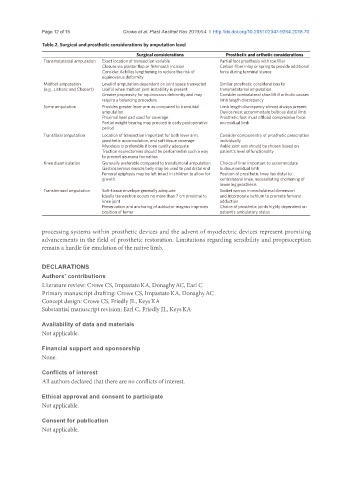
Table 2. Surgical and prosthetic considerations by amputation level
Surgical considerations Prosthetic and orthotic considerations
Transmetatarsal amputation Exact location of transection variable Partial foot prosthesis with toe filler
Closure via plantar flap or fishmouth incision Carbon-fiber inlay or spring to provide additional
Consider Achilles lengthening to reduce the risk of force during terminal stance
equinovarus deformity
Midfoot amputation Level of amputation dependent on joint space transected Similar prosthetic considerations to
(e.g., Lisfranc and Chopart) Useful when midfoot joint instability is present transmetatarsal amputation
Greater propensity for equinovarus deformity and may Consider contralateral shoe lift if orthotic causes
require a balancing procedure limb length discrepancy
Syme amputation Provides greater lever arm as compared to transtibial Limb length discrepancy almost always present
amputation Device must accommodate bulbous distal limb
Proximal heel pad used for coverage Prosthetic foot must offload compressive force
Partial weight bearing may proceed in early postoperative on residual limb
period
Transtibial amputation Location of transection important for both lever arm, Consider componentry of prosthetic prescription
prosthetic accomodation, and soft tissue coverage individually
Myodesis is preferable if bone quality adequate Ankle joint axis should be chosen based on
Traction neurectomies should be performed in such a way patient’s level of functionality
to prevent neuroma formation
Knee disarticulation Generally preferable compared to transfemoral amputation Choice of liner important to accommodate
Gastrocnemius muscle belly may be used to pad distal end bulbous residual limb
Femoral epiphysis may be left intact in children to allow for Position of prosthetic knee lies distal to
growth contralateral knee, necessitating shortening of
lower leg prosthesis
Transfemoral amputation Soft-tissue envelope generally adequate Socket narrow in mediolateral dimension
Ideally transection occurs no more than 7 cm proximal to and incorporate ischium to promote femoral
knee joint adduction
Preservation and anchoring of adductor magnus improves Choice of prosthetic joints highly dependent on
position of femur patient’s ambulatory status
processing systems within prosthetic devices and the advent of myoelectric devices represent promising
advancements in the field of prosthetic restoration. Limitations regarding sensibility and proprioception
remain a hurdle for emulation of the native limb.
DECLARATIONS
Authors’ contributions
Literature review: Crowe CS, ImpastatoKA, DonaghyAC, Earl C
Primary manuscript drafting: Crowe CS, ImpastatoKA, DonaghyAC
Concept design: Crowe CS, Friedly JL, KeysKA
Substantial manuscript revision: Earl C, Friedly JL, KeysKA
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.