
Page 25 - Read Online
P. 25
Page 14 of 22 Ballestri et al. Metab Target Organ Damage 2023;3:1 https://dx.doi.org/10.20517/mtod.2022.23
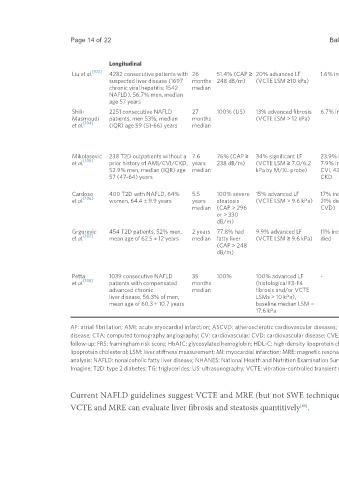
Longitudinal
[103]
Liu et al. 4282 consecutive patients with 26 51.4% (CAP ≥ 20% advanced LF 1.6% incident CVE LSM predicted liver-related events but not CVEs. Age, sex, platelet count, serum
suspected liver disease (1697 months 248 dB/m) (VCTE LSM ≥10 kPa) Subgroup analyses of viral hepatitis and NAFLD albumin, creatinine, cardiometabolic
chronic viral hepatitis; 1542 median patients revealed similar results risk factors, diabetes-related
NAFLD), 56.7% men, median variables
age 57 years
Shili- 2251 consecutive NAFLD 27 100% (US) 13% advanced fibrosis 6.7% incident CVE LSM independently predicted overall survival Age, gender, BMI, MetS, diabetes,
Masmoudi patients, men 53%, median months (VCTE LSM > 12 kPa) (HR 2.85, 95%CI: 1.65-4.92). Patients with hypertension, abdominal obesity,
[104]
et al. (IQR) age 59 (51-66) years median elevated LSM presented significantly more CVEs low HDL-C, high TG
and liver events but not cancers
LSM was as accurate as a clinical model to
predict overall survival and CVEs
Mikolasevic 238 T2D outpatients without a 7.6 76% (CAP ≥ 34% significant LF 23.9% incident AMI, Elevated CAP (HR 2.34) and elevated LSM (HR Traditional CV risk factors and
[105]
et al. prior history of AMI/CVI/CKD, years 238 dB/m) (VCTE LSM ≥ 7.0/6.2 7.9% incident 2.84), independently of each other, were diabetes-related variables
52.9% men, median (IQR) age median kPa by M/XL probe) CVI, 42.4% incident associated with a higher risk of developing the
57 (47-64) years CKD composite outcome (AMI, CVI, or CKD), as well
as incident AMI or CKD alone
Cardoso 400 T2D with NAFLD, 64% 5.5 100% severe 15% advanced LF 17% incident CVE An increasing LSM was a risk marker for total Age, sex, smoking, cardiometabolic
[106]
et al. women, 64.4 ± 9.9 years years steatosis (VCTE LSM > 9.6 kPa) 21% died (47% from CVEs (HR 1.05) and all-cause mortality (HR: risk factors, diabetes-related
median (CAP > 296 CVD) 1.04). If LSM > 9.6 kPa: HR 2.66 for total CVEs, variables, ASCVD, microvascular
or > 330 3.03 for MCVEs, 1.7 for all-cause mortality, and complications at baseline, use of
dB/m) 2.46 for CV mortality statins and aspirin
Grgurevic 454 T2D patients, 52% men, 2 years 77.8% had 9.9% advanced LF 11% incident CVE 3.7% Age and platelet count (but not FIB-4, LSM, and -
[107]
et al. mean age of 62.5 ± 12 years median fatty liver (VCTE LSM ≥ 9.6 kPa) died CAP) independently predicted poor outcomes.
(CAP > 248 This study found that no liver-related
dB/m) morbidity/mortality may virtually mirror a low
prevalence of advanced LF, probably overrated
by using a 9.6 LSM cut-off
Petta 1039 consecutive NAFLD 35 100% 100% advanced LF - In 533 patients with available LSMs during the Age, gender, BMI, presence of Child-
[108]
et al. patients with compensated months (histological F3-F4 follow-up period, change in LSM was Pugh A6, platelets and baseline LSM
advanced chronic median fibrosis and/or VCTE independently associated with overall mortality
liver disease, 56.3% of men, LSMs > 10 kPa), (HR 1.73) and liver-related mortality (HR 1.96).
mean age of 60.3 ± 10.7 years baseline median LSM = LSM did not predict extra-hepatic events
17.6 kPa occurrence at univariate analysis
AF: atrial fibrillation; AMI: acute myocardial infarction; ASCVD: atherosclerotic cardiovascular diseases; BMI: body mass index; CAC: coronary artery calcium; CHD: coronary heart disease; CKD: chronic kidney
disease; CTA: computed tomography angiography; CV: cardiovascular; CVD: cardiovascular disease; CVE: cardiovascular event; CVI: cerebrovascular insult (i.e. ischemic stroke or transient ischemic attack); F-up:
follow-up; FRS: framingham risk score; HbA1C: glycosylated hemoglobin; HDL-C: high-density lipoprotein cholesterol; HR: hazard ratio; IQR: interquartile range; IS: ischemic stroke; kPa: kilopascal; LDL-C: low-density
lipoprotein cholesterol; LSM: liver stiffness measurement; MI: myocardial infarction; MRE: magnetic resonance elastography; MRI-PDFF: Magnetic Resonance Imaging Proton Density Fat Fraction; MVA: multivariate
analysis: NAFLD: nonalcoholic fatty liver disease; NHANES: National Health and Nutrition Examination Survey; SBP: systolic blood pressure; 2DSWE-SSI: two-dimensional point shear wave elastography-SuperSonic
Imagine; T2D: type 2 diabetes; TG: triglycerides; US: ultrasonography; VCTE: vibration-controlled transient elastography; -: not applicable/available.
Current NAFLD guidelines suggest VCTE and MRE (but not SWE techniques) for LSM because no NAFLD follow-up studies have used SWE; moreover,
VCTE and MRE can evaluate liver fibrosis and steatosis quantitively .
[80]