
Page 507 - Read Online
P. 507
Page 14 of 17 Cannata et al. Mini-invasive Surg 2020;4:53 I http://dx.doi.org/10.20517/2574-1225.2020.41
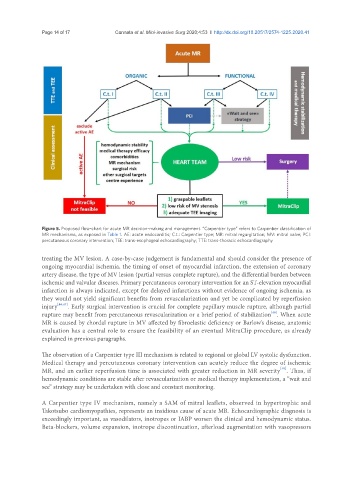
Figure 5. Proposed flow-chart for acute MR decision-making and management. “Carpentier type” refers to Carpentier classification of
MR mechanisms, as exposed in Table 1. AE: acute endocarditis; C.t.: Carpentier type; MR: mitral regurgitation; MV: mitral valve; PCI:
percutaneous coronary intervention; TEE: trans-esophageal echocardiography; TTE: trans-thoracic echocardiography
treating the MV lesion. A case-by-case judgement is fundamental and should consider the presence of
ongoing myocardial ischemia, the timing of onset of myocardial infarction, the extension of coronary
artery disease, the type of MV lesion (partial versus complete rupture), and the differential burden between
ischemic and valvular diseases. Primary percutaneous coronary intervention for an ST-elevation myocardial
infarction is always indicated, except for delayed infarctions without evidence of ongoing ischemia, as
they would not yield significant benefits from revascularization and yet be complicated by reperfusion
injury [46,47] . Early surgical intervention is crucial for complete papillary muscle rupture, although partial
[48]
rupture may benefit from percutaneous revascularization or a brief period of stabilization . When acute
MR is caused by chordal rupture in MV affected by fibroelastic deficiency or Barlow’s disease, anatomic
evaluation has a central role to ensure the feasibility of an eventual MitraClip procedure, as already
explained in previous paragraphs.
The observation of a Carpentier type III mechanism is related to regional or global LV systolic dysfunction.
Medical therapy and percutaneous coronary intervention can acutely reduce the degree of ischemic
[49]
MR, and an earlier reperfusion time is associated with greater reduction in MR severity . Thus, if
hemodynamic conditions are stable after revascularization or medical therapy implementation, a “wait and
see” strategy may be undertaken with close and constant monitoring.
A Carpentier type IV mechanism, namely a SAM of mitral leaflets, observed in hypertrophic and
Takotsubo cardiomyopathies, represents an insidious cause of acute MR. Echocardiographic diagnosis is
exceedingly important, as vasodilators, inotropes or IABP worsen the clinical and hemodynamic status.
Beta-blockers, volume expansion, inotrope discontinuation, afterload augmentation with vasopressors