
Page 451 - Read Online
P. 451
Scotti et al. Mini-invasive Surg 2020;4:49 I http://dx.doi.org/10.20517/2574-1225.2020.38 Page 5 of 9
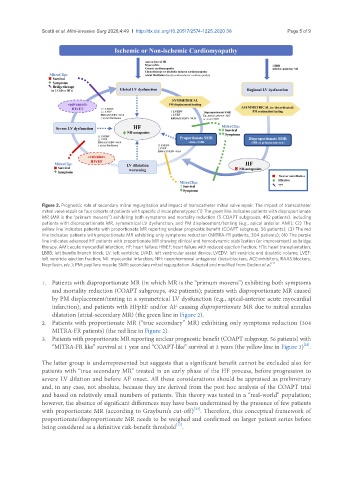
Figure 2. Prognostic role of secondary mitral regurgitation and impact of transcatheter mitral valve repair. The impact of transcatheter
mitral valve repair on four cohorts of patients with specific clinical phenotypes: (1) The green line indicates patients with disproportionate
MR (MR is the “primum movens”) exhibiting both symptoms and mortality reduction (5 COAPT subgroups, 492 patients), including
patients with disproportionate MR, symmetrical LV dysfunction, and PM displacement/tenting (e.g., apical anterior AMI); (2) The
yellow line indicates patients with proportionate MR reporting unclear prognostic benefit (COAPT subgroup, 56 patients); (3) The red
line indicates patients with proportionate MR exhibiting only symptoms reduction (MITRA-FR patients, 304 patients); (4) The purple
line indicates advanced HF patients with proportionate MR showing clinical and hemodynamic stabilization (or improvement) as bridge
therapy. AMI: acute myocardial infarction; HF: heart failure; HFrEF: heart failure with reduced ejection fraction; HTx: heart transplantation;
LBBB: left bundle branch block; LV: left ventricle; LVAD: left ventricular assist device; LVEDV: left ventricle end diastolic volume; LVEF:
left ventricle ejection fraction; MI: myocardial infarction; NH: neurohormonal antagonist (beta-blockers, ACE-inhibitors, RAAS blockers,
Neprilysin, etc.); PM: papillary muscle; SMR: secondary mitral regurgitation. Adapted and modified from Godino et al. [7]
1. Patients with disproportionate MR (in which MR is the “primum movens”) exhibiting both symptoms
and mortality reduction (COAPT subgroups, 492 patients); patients with disproportionate MR caused
by PM displacement/tenting in a symmetrical LV dysfunction (e.g., apical-anterior acute myocardial
infarction); and patients with HFpEF and/or AF causing disproportionate MR due to mitral annulus
dilatation (atrial-secondary MR) (the green line in Figure 2).
2. Patients with proportionate MR (“true secondary” MR) exhibiting only symptoms reduction (304
MITRA-FR patients) (the red line in Figure 2).
3. Patients with proportionate MR reporting unclear prognostic benefit (COAPT subgroup, 56 patients) with
[21]
“MITRA-FR like” survival at 1 year and “COAPT-like” survival at 2 years (the yellow line in Figure 2) .
The latter group is underrepresented but suggests that a significant benefit cannot be excluded also for
patients with “true secondary MR” treated in an early phase of the HF process, before progression to
severe LV dilation and before AF onset. All these considerations should be appraised as preliminary
and, in any case, not absolute, because they are derived from the post hoc analysis of the COAPT trial
and based on relatively small numbers of patients. This theory was tested in a “real-world” population;
however, the absence of significant differences may have been undermined by the presence of few patients
[22]
with proportionate MR (according to Grayburn’s cut-off) . Therefore, this conceptual framework of
proportionate/disproportionate MR needs to be weighed and confirmed on larger patient series before
[17]
being considered as a definitive risk-benefit threshold .