
Page 39 - Read Online
P. 39
Ohmura et al. Mini-invasive Surg 2019;3:4 I http://dx.doi.org/10.20517/2574-1225.2018.69 Page 5 of 13
A B C
D E F
G H I
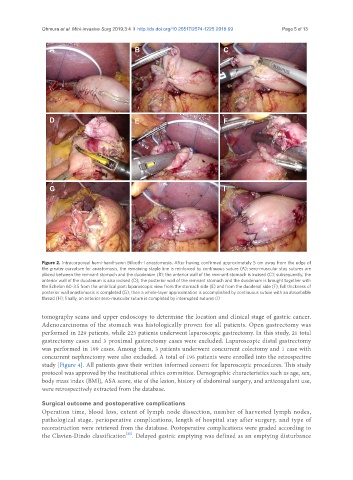
Figure 2. Intracorporeal hemi-hand-sewn Billroth-I anastomosis. After having confirmed approximately 5 cm away from the edge of
the greater curvature for anastomosis, the remaining staple line is reinforced by continuous suture (A); sero-muscular stay sutures are
placed between the remnant stomach and the duodenum (B); the anterior wall of the remnant stomach is incised (C); subsequently, the
anterior wall of the duodenum is also incised (D); the posterior wall of the remnant stomach and the duodenum is brought together with
the Echelon 60-3.5 from the umbilical port: laparoscopic view from the stomach side (E) and from the duodenal side (F); full thickness of
posterior wall anastomosis is completed (G); then a whole-layer approximation is accomplished by continuous suture with an absorbable
thread (H); finally, an anterior sero-muscular suture is completed by interrupted sutures (I)
tomography scans and upper endoscopy to determine the location and clinical stage of gastric cancer.
Adenocarcinoma of the stomach was histologically proven for all patients. Open gastrectomy was
performed in 229 patients, while 223 patients underwent laparoscopic gastrectomy. In this study, 21 total
gastrectomy cases and 3 proximal gastrectomy cases were excluded. Laparoscopic distal gastrectomy
was performed in 199 cases. Among them, 3 patients underwent concurrent colectomy and 1 case with
concurrent nephrectomy were also excluded. A total of 195 patients were enrolled into the retrospective
study [Figure 4]. All patients gave their written informed consent for laparoscopic procedures. This study
protocol was approved by the institutional ethics committee. Demographic characteristics such as age, sex,
body mass index (BMI), ASA score, site of the lesion, history of abdominal surgery, and anticoagulant use,
were retrospectively extracted from the database.
Surgical outcome and postoperative complications
Operation time, blood loss, extent of lymph node dissection, number of harvested lymph nodes,
pathological stage, perioperative complications, length of hospital stay after surgery, and type of
reconstruction were retrieved from the database. Postoperative complications were graded according to
[20]
the Clavien-Dindo classification . Delayed gastric emptying was defined as an emptying disturbance