
Page 296 - Read Online
P. 296
Jeong et al. Mini-invasive Surg 2019;3:38 I http://dx.doi.org/10.20517/2574-1225.2019.42 Page 9 of 11
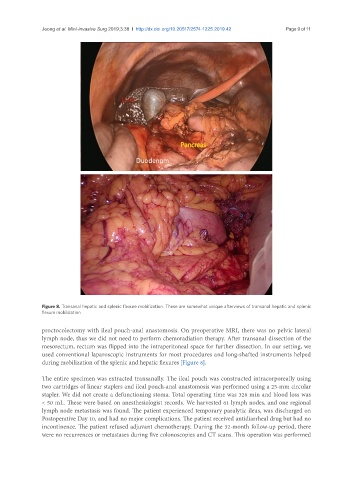
Figure 8. Transanal hepatic and splenic flexure mobilization. These are somewhat unique afterviews of transanal hepatic and splenic
flexure mobilization
proctocolectomy with ileal pouch-anal anastomosis. On preoperative MRI, there was no pelvic lateral
lymph node, thus we did not need to perform chemoradiation therapy. After transanal dissection of the
mesorectum, rectum was flipped into the intraperitoneal space for further dissection. In our setting, we
used conventional laparoscopic instruments for most procedures and long-shafted instruments helped
during mobilization of the splenic and hepatic flexures [Figure 8].
The entire specimen was extracted transanally. The ileal pouch was constructed intracorporeally using
two cartridges of linear staplers and ileal pouch-anal anastomosis was performed using a 25-mm circular
stapler. We did not create a defunctioning stoma. Total operating time was 328 min and blood loss was
< 50 mL. These were based on anesthesiologist records. We harvested 61 lymph nodes, and one regional
lymph node metastasis was found. The patient experienced temporary paralytic ileus, was discharged on
Postoperative Day 10, and had no major complications. The patient received antidiarrheal drug but had no
incontinence. The patient refused adjuvant chemotherapy. During the 32-month follow-up period, there
were no recurrences or metastases during five colonoscopies and CT scans. This operation was performed