
Page 284 - Read Online
P. 284
Page 8 of 11 Serra-Aracil et al. Mini-invasive Surg 2019;3:37 I http://dx.doi.org/10.20517/2574-1225.2019.36
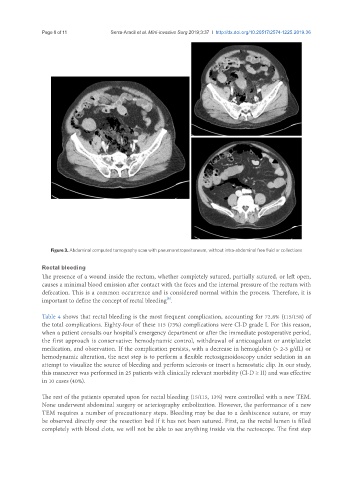
Figure 3. Abdominal computed tomography scan with pneumoretroperitoneum, without intra-abdominal free fluid or collections
Rectal bleeding
The presence of a wound inside the rectum, whether completely sutured, partially sutured, or left open,
causes a minimal blood emission after contact with the feces and the internal pressure of the rectum with
defecation. This is a common occurrence and is considered normal within the process. Therefore, it is
[6]
important to define the concept of rectal bleeding .
Table 4 shows that rectal bleeding is the most frequent complication, accounting for 72.8% (115/158) of
the total complications. Eighty-four of these 115 (73%) complications were Cl-D grade I. For this reason,
when a patient consults our hospital’s emergency department or after the immediate postoperative period,
the first approach is conservative: hemodynamic control, withdrawal of anticoagulant or antiplatelet
medication, and observation. If the complication persists, with a decrease in hemoglobin (> 2-3 g/dL) or
hemodynamic alteration, the next step is to perform a flexible rectosigmoidoscopy under sedation in an
attempt to visualize the source of bleeding and perform sclerosis or insert a hemostatic clip. In our study,
this maneuver was performed in 25 patients with clinically relevant morbidity (Cl-D ≥ II) and was effective
in 10 cases (40%).
The rest of the patients operated upon for rectal bleeding (15/115, 13%) were controlled with a new TEM.
None underwent abdominal surgery or arteriography embolization. However, the performance of a new
TEM requires a number of precautionary steps. Bleeding may be due to a deshiscence suture, or may
be observed directly over the resection bed if it has not been sutured. First, as the rectal lumen is filled
completely with blood clots, we will not be able to see anything inside via the rectoscope. The first step