
Page 32 - Read Online
P. 32
Page 6 of 9 Kitamura et al. Mini-invasive Surg 2022;6:44 https://dx.doi.org/10.20517/2574-1225.2022.27
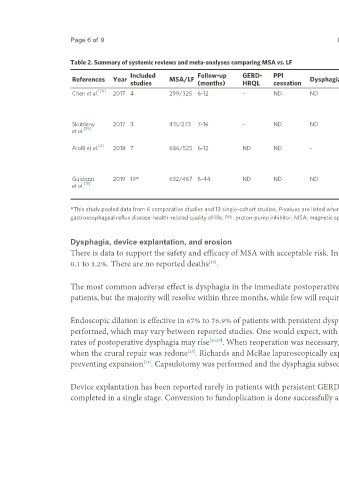
Table 2. Summary of systemic reviews and meta-analyses comparing MSA vs. LF
Included Follow-up GERD- PPI Endoscopic MSA MSA
References Year MSA/LF Dysphagia Belching Vomiting Gas bloat Reoperation
studies (months) HRQL cessation dilation erosion removal
[26]
Chen et al. 2017 4 299/325 6-12 - ND ND ND ND ND RR: 0.71 ND - -
95%CI:
0.54-0.94
P = 0.02
Skubleny 2017 3 415/273 7-16 - ND ND ND 95.2 MSA 93.5% vs. ND - - -
[29]
et al. 65.9% LF 49.5%
P < 0.00001 P < 0.0001
[2]
Aiolfi et al. 2018 7 686/525 6-12 ND ND - ND OR: 5.53 OR: 10.10 OR: 0.39 ND - -
95%CI: 3.73- 95%CI: 5.33- 95%CI:
8.19 19.15 0.25-0.61
P < 0.001 P < 0.001 P < 0.001
Guidozzi 2019 19* 632/467 6-44 ND ND ND - OR: 12.34 - OR: 0.34 ND 0.30% 3.30%
[19]
et al. 95%CI: 6.43- 95CI: 0.16-
23.7 0.71
*This study pooled data from 6 comparative studies and 13 single-cohort studies. P-values are listed when reported for significant differences in reported symptoms. LF: Laparoscopic fundoplication; GERD-HRQL:
gastroesophageal reflux disease-health-related quality of life; PPI: proton-pump inhibitor; MSA: magnetic sphincter augmentation; ND: no difference; OR: odd’s ratio; RR: relative risk.
Dysphagia, device explantation, and erosion
There is data to support the safety and efficacy of MSA with acceptable risk. Intraoperative complications are 0.1%, explantation of 1.1 to 6.7%, and erosion of
0.1 to 1.2%. There are no reported deaths .
[18]
The most common adverse effect is dysphagia in the immediate postoperative period, which is 43% to 83%. Persistent dysphagia may occur in up to 19% of
patients, but the majority will resolve within three months, while few will require endoscopic dilation [28,29] .
Endoscopic dilation is effective in 67% to 76.9% of patients with persistent dysphagia . This may be due to non-standardization of whether the crural repair is
[18]
performed, which may vary between reported studies. One would expect, with newer studies incorporating larger hiatal hernias and complicated reflux cases,
rates of postoperative dysphagia may rise [20,30] . When reoperation was necessary, a crural closure was noted to be the culprit in one case and symptoms resolved
when the crural repair was redone . Richards and McRae laparoscopically explored two patients and found the MSA device was encapsulated in scar tissue,
[23]
preventing expansion . Capsulotomy was performed and the dysphagia subsequently resolved.
[13]
Device explantation has been reported rarely in patients with persistent GERD or dysphagia. In those instances, device removal has been uncomplicated and
completed in a single stage. Conversion to fundoplication is done successfully and authors feel relatively easy given the limited dissection needed for MSA [13,23] .