
Page 71 - Read Online
P. 71
Page 12 of 22 Gharagozloo et al. Mini-invasive Surg 2020;4:66 I http://dx.doi.org/10.20517/2574-1225.2020.53
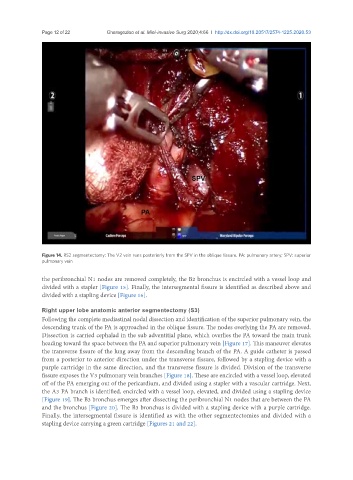
Figure 14. RS2 segmentectomy: The V2 vein runs posteriorly from the SPV in the oblique fissure. PA: pulmonary artery; SPV: superior
pulmonary vein
the peribronchial N1 nodes are removed completely, the B2 bronchus is encircled with a vessel loop and
divided with a stapler [Figure 15]. Finally, the intersegmental fissure is identified as described above and
divided with a stapling device [Figure 16].
Right upper lobe anatomic anterior segmentectomy (S3)
Following the complete mediastinal nodal dissection and identification of the superior pulmonary vein, the
descending trunk of the PA is approached in the oblique fissure. The nodes overlying the PA are removed.
Dissection is carried cephalad in the sub adventitial plane, which overlies the PA toward the main trunk
heading toward the space between the PA and superior pulmonary vein [Figure 17]. This maneuver elevates
the transverse fissure of the lung away from the descending branch of the PA. A guide catheter is passed
from a posterior to anterior direction under the transverse fissure, followed by a stapling device with a
purple cartridge in the same direction, and the transverse fissure is divided. Division of the transverse
fissure exposes the V3 pulmonary vein branches [Figure 18]. These are encircled with a vessel loop, elevated
off of the PA emerging out of the pericardium, and divided using a stapler with a vascular cartridge. Next,
the A3 PA branch is identified, encircled with a vessel loop, elevated, and divided using a stapling device
[Figure 19]. The B3 bronchus emerges after dissecting the peribronchial N1 nodes that are between the PA
and the bronchus [Figure 20]. The B3 bronchus is divided with a stapling device with a purple cartridge.
Finally, the intersegmental fissure is identified as with the other segmentectomies and divided with a
stapling device carrying a green cartridge [Figures 21 and 22].