
Page 68 - Read Online
P. 68
Gharagozloo et al. Mini-invasive Surg 2020;4:66 I http://dx.doi.org/10.20517/2574-1225.2020.53 Page 9 of 22
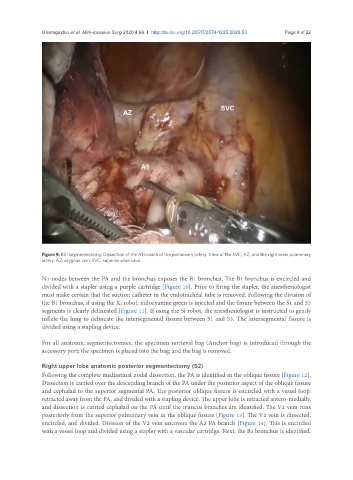
Figure 9. RS1 segmentectomy: Dissection of the A1 branch of the pulmonary artery. View of the SVC, AZ, and the right main pulmonary
artery. AZ: azygous vein; SVC: superior vena cava
N1 nodes between the PA and the bronchus exposes the B1 bronchus. The B1 bronchus is encircled and
divided with a stapler using a purple cartridge [Figure 10]. Prior to firing the stapler, the anesthesiologist
must make certain that the suction catheter in the endotracheal tube is removed. Following the division of
the B1 bronchus, if using the Xi robot, indocyanine green is injected and the fissure between the S1 and S3
segments is clearly delineated [Figure 11]. If using the Si robot, the anesthesiologist is instructed to gently
inflate the lung to delineate the intersegmental fissure between S1 and S3. The intersegmental fissure is
divided using a stapling device.
For all anatomic segmentectomies, the specimen retrieval bag (Anchor bag) is introduced through the
accessory port; the specimen is placed into the bag; and the bag is removed.
Right upper lobe anatomic posterior segmentectomy (S2)
Following the complete mediastinal nodal dissection, the PA is identified in the oblique fissure [Figure 12].
Dissection is carried over the descending branch of the PA under the posterior aspect of the oblique fissure
and cephalad to the superior segmental PA. The posterior oblique fissure is encircled with a vessel loop,
retracted away from the PA, and divided with a stapling device. The upper lobe is retracted antero-medially,
and dissection is carried cephalad on the PA until the truncus branches are identified. The V2 vein runs
posteriorly from the superior pulmonary vein in the oblique fissure [Figure 13]. The V2 vein is dissected,
encircled, and divided. Division of the V2 vein uncovers the A2 PA branch [Figure 14]. This is encircled
with a vessel loop and divided using a stapler with a vascular cartridge. Next, the B2 bronchus is identified,