
Page 159 - Read Online
P. 159
Page 4 of 9 Sollie et al. Mini-invasive Surg 2020;4:80 I http://dx.doi.org/10.20517/2574-1225.2020.81
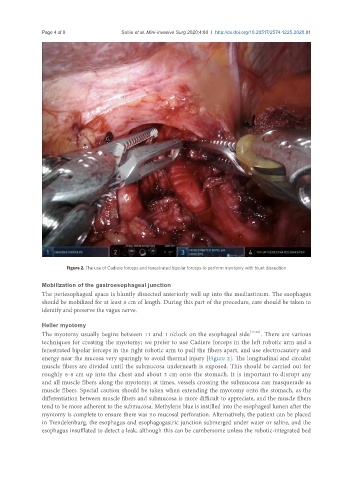
Figure 2. The use of Cadiere forceps and fenestrated bipolar forceps to perform myotomy with blunt dissection
Mobilization of the gastroesophageal junction
The periesophageal space is bluntly dissected anteriorly well up into the mediastinum. The esophagus
should be mobilized for at least 8 cm of length. During this part of the procedure, care should be taken to
identify and preserve the vagus nerve.
Heller myotomy
The myotomy usually begins between 11 and 1 o’clock on the esophageal side [17,26] . There are various
techniques for creating the myotomy; we prefer to use Cadiere forceps in the left robotic arm and a
fenestrated bipolar forceps in the right robotic arm to pull the fibers apart, and use electrocautery and
energy near the mucosa very sparingly to avoid thermal injury [Figure 2]. The longitudinal and circular
muscle fibers are divided until the submucosa underneath is exposed. This should be carried out for
roughly 6-8 cm up into the chest and about 3 cm onto the stomach. It is important to disrupt any
and all muscle fibers along the myotomy; at times, vessels crossing the submucosa can masquerade as
muscle fibers. Special caution should be taken when extending the myotomy onto the stomach, as the
differentiation between muscle fibers and submucosa is more difficult to appreciate, and the muscle fibers
tend to be more adherent to the submucosa. Methylene blue is instilled into the esophageal lumen after the
myotomy is complete to ensure there was no mucosal perforation. Alternatively, the patient can be placed
in Trendelenburg, the esophagus and esophagogastric junction submerged under water or saline, and the
esophagus insufflated to detect a leak, although this can be cumbersome unless the robotic-integrated bed