
Page 135 - Read Online
P. 135
Gharagozloo et al. Mini-invasive Surg 2020;4:48 I http://dx.doi.org/10.20517/2574-1225.2020.35 Page 13 of 19
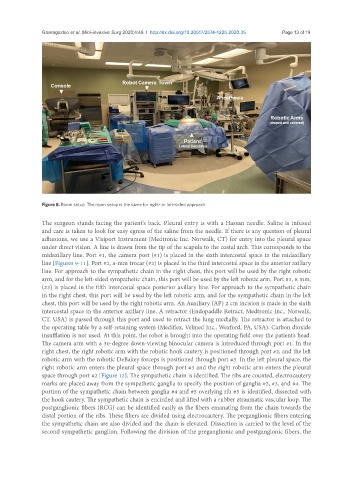
Figure 8. Room setup. The room setup is the same for right- or left-sided approach
The surgeon stands facing the patient’s back. Pleural entry is with a Hassan needle. Saline is infused
and care is taken to look for easy egress of the saline from the needle. If there is any question of pleural
adhesions, we use a Visiport Instrument (Medtronic Inc. Norwalk, CT) for entry into the pleural space
under direct vision. A line is drawn from the tip of the scapula to the costal arch. This corresponds to the
midaxillary line. Port #1, the camera port (#1) is placed in the sixth intercostal space in the midaxillary
line [Figures 9-11]. Port #2, 8-mm trocar (#2) is placed in the third intercostal space in the anterior axillary
line. For approach to the sympathetic chain in the right chest, this port will be used by the right robotic
arm, and for the left-sided sympathetic chain, this port will be used by the left robotic arm. Port #3, 8 mm,
(#3) is placed in the fifth intercostal space posterior axillary line. For approach to the sympathetic chain
in the right chest, this port will be used by the left robotic arm, and for the sympathetic chain in the left
chest, this port will be used by the right robotic arm. An Auxiliary (AP) 2 cm incision is made in the sixth
intercostal space in the anterior axillary line. A retractor (Endopaddle Retract, Medtronic Inc., Norwalk,
CT. USA) is passed through this port and used to retract the lung medially. The retractor is attached to
the operating table by a self-retaining system (Mediflex, Velmed Inc., Wexford, PA, USA). Carbon dioxide
insufflation is not used. At this point, the robot is brought into the operating field over the patient’s head.
The camera arm with a 30-degree down-viewing binocular camera is introduced through port #1. In the
right chest, the right robotic arm with the robotic hook cautery is positioned through port #2, and the left
robotic arm with the robotic DeBakey forceps is positioned through port #3. In the left pleural space, the
right robotic arm enters the pleural space through port #3 and the right robotic arm enters the pleural
space through port #2 [Figure 12]. The sympathetic chain is identified. The ribs are counted, electrocautery
marks are placed away from the sympathetic ganglia to specify the position of ganglia #2, #3, and #4. The
portion of the sympathetic chain between ganglia #4 and #5 overlying rib #5 is identified, dissected with
the hook cautery. The sympathetic chain is encircled and lifted with a rubber atraumatic vascular loop. The
postganglionic fibers (RCG) can be identified easily as the fibers emanating from the chain towards the
distal portion of the ribs. These fibers are divided using electrocautery. The preganglionic fibers entering
the sympathetic chain are also divided and the chain is elevated. Dissection is carried to the level of the
second sympathetic ganglion. Following the division of the preganglionic and postganglonic fibers, the