
Page 36 - Read Online
P. 36
Page 4 of 6 Zirafa et al. Mini-invasive Surg 2020;4:13 I http://dx.doi.org/10.20517/2574-1225.2019.35
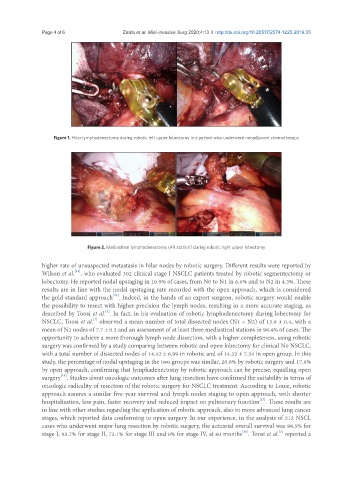
Figure 1. Hilar lymphadenectomy during robotic left upper lobectomy in a patient who underwent neoadjuvant chemotherapy
Figure 2. Mediastinal lymphadenectomy (4R station) during robotic right upper lobectomy
higher rate of unsuspected metastasis in hilar nodes by robotic surgery. Different results were reported by
[13]
Wilson et al. , who evaluated 302 clinical stage I NSCLC patients treated by robotic segmentectomy or
lobectomy. He reported nodal upstaging in 10.9% of cases, from N0 to N1 in 6.6% and to N2 in 4.3%. These
results are in line with the nodal upstaging rate recorded with the open approach, which is considered
[13]
the gold standard approach . Indeed, in the hands of an expert surgeon, robotic surgery would enable
the possibility to resect with higher precision the lymph nodes, resulting in a more accurate staging, as
described by Toosi et al. . In fact, in his evaluation of robotic lymphadenectomy during lobectomy for
[3]
[3]
NSCLC, Toosi et al. observed a mean number of total dissected nodes (N1 + N2) of 13.9 ± 0.4, with a
mean of N2 nodes of 7.7 ± 0.3 and an assessment of at least three mediastinal stations in 98.4% of cases. The
opportunity to achieve a more thorough lymph node dissection, with a higher completeness, using robotic
surgery was confirmed by a study comparing between robotic and open lobectomy for clinical N0 NSCLC,
with a total number of dissected nodes of 14.42 ± 6.99 in robotic and of 14.32 ± 7.34 in open group. In this
study, the percentage of nodal upstaging in the two groups was similar, 20.8% by robotic surgery and 17.9%
by open approach, confirming that lymphadenectomy by robotic approach can be precise, equalling open
surgery . Studies about oncologic outcomes after lung resection have confirmed the suitability in terms of
[14]
oncologic radicality of resection of the robotic surgery for NSCLC treatment. According to Louie, robotic
approach assures a similar five-year survival and lymph nodes staging to open approach, with shorter
[15]
hospitalization, less pain, faster recovery and reduced impact on pulmonary function . These results are
in line with other studies regarding the application of robotic approach, also in more advanced lung cancer
stages, which reported data conforming to open surgery. In our experience, in the analysis of 212 NSCL
cases who underwent major lung resection by robotic surgery, the actuarial overall survival was 98.5% for
[3]
[16]
stage I, 93.7% for stage II, 73.1% for stage III and 0% for stage IV, at 60 months . Toosi et al. reported a