
Page 12 - Read Online
P. 12
Matto et al. Mini-invasive Surg. 2025;9:19 https://dx.doi.org/10.20517/2574-1225.2025.51 Page 3 of 11
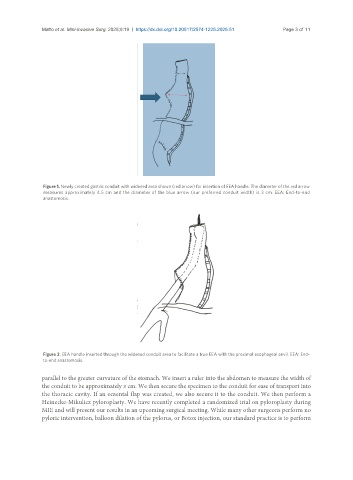
Figure 1. Newly created gastric conduit with widened area shown (red arrow) for insertion of EEA handle. The diameter of the red arrow
measures approximately 4.5 cm and the diameter of the blue arrow (our preferred conduit width) is 3 cm. EEA: End-to-end
anastomosis.
Figure 2. EEA handle inserted through the widened conduit area to facilitate a true EEA with the proximal esophageal anvil. EEA: End-
to-end anastomosis.
parallel to the greater curvature of the stomach. We insert a ruler into the abdomen to measure the width of
the conduit to be approximately 3 cm. We then secure the specimen to the conduit for ease of transport into
the thoracic cavity. If an omental flap was created, we also secure it to the conduit. We then perform a
Heinecke-Mikulicz pyloroplasty. We have recently completed a randomized trial on pyloroplasty during
MIE and will present our results in an upcoming surgical meeting. While many other surgeons perform no
pyloric intervention, balloon dilation of the pylorus, or Botox injection, our standard practice is to perform