
Page 46 - Read Online
P. 46
Sullivan et al. Mini-invasive Surg 2023;7:15 https://dx.doi.org/10.20517/2574-1225.2022.106 Page 3 of 11
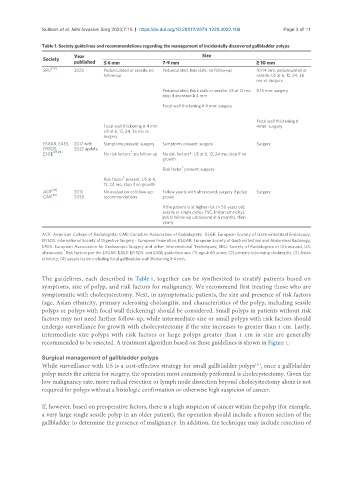
Table 1. Society guidelines and recommendations regarding the management of incidentally discovered gallbladder polyps
Society Year Size
published ≤ 6 mm 7-9 mm ≥ 10 mm
SRU [26] 2022 Pedunculated or sessile: no Pedunculated, thin stalk: no follow-up 10-14 mm, pedunculated or
follow-up sessile: US at 6, 12, 24, 36
mo vs. surgery
Pedunculated, thick stalk or sessile: US at 12 mo, ≥ 15 mm: surgery
stop if decrease ≥ 4 mm
Focal wall thickening ≥ 4 mm: surgery
Focal wall thickening ≥
Focal wall thickening ≥ 4 mm: 4mm: surgery
US at 6, 12, 24, 36 mo vs.
surgery
ESGAR, EAES, 2017 with Symptoms present: surgery Symptoms present: surgery Surgery
EFISDS, 2022 update
*
ESGE [27,28] No risk factors : no follow-up No risk factors*: US at 6, 12, 24 mo; stop if no
growth
*
Risk factor present: surgery
*
Risk factor present: US at 6,
12, 24 mo; stop if no growth
[29]
ACR 2013 No evaluation or follow-up Follow yearly with ultrasound; surgery if polyp Surgery
CAR [30] 2020 recommendations grows
If the patient is at higher risk (> 50 years old,
sessile or single polyp, PSC, Indian ethnicity),
initial follow-up ultrasound at 6 months, then
yearly
ACR: American College of Radiologists; CAR: Canadian Association of Radiologists; ESGE: European Society of Gastrointestinal Endoscopy;
EFISDS: International Society of Digestive Surgery - European Federation; ESGAR: European Society of Gastrointestinal and Abdominal Radiology;
EAES: European Association for Endoscopic Surgery and other Interventional Techniques; SRU: Society of Radiologists in Ultrasound; US:
*
ultrasound; Risk factors per the ESGAR: EAES: EFISDS: and ESGE guidelines are: (1) age ≥ 60 years; (2) primary sclerosing cholangitis; (3) Asian
ethnicity; (4) sessile lesion including focal gallbladder wall thickening ≥ 4 mm.
The guidelines, each described in Table 1, together can be synthesized to stratify patients based on
symptoms, size of polyp, and risk factors for malignancy. We recommend first treating those who are
symptomatic with cholecystectomy. Next, in asymptomatic patients, the size and presence of risk factors
(age, Asian ethnicity, primary sclerosing cholangitis, and characteristics of the polyp, including sessile
polyps or polyps with focal wall thickening) should be considered. Small polyps in patients without risk
factors may not need further follow-up, while intermediate-size or small polyps with risk factors should
undergo surveillance for growth with cholecystectomy if the size increases to greater than 1 cm. Lastly,
intermediate-size polyps with risk factors or large polyps greater than 1 cm in size are generally
recommended to be resected. A treatment algorithm based on these guidelines is shown in Figure 1.
Surgical management of gallbladder polyps
[31]
While surveillance with US is a cost-effective strategy for small gallbladder polyps , once a gallbladder
polyp meets the criteria for surgery, the operation most commonly performed is cholecystectomy. Given the
low malignancy rate, more radical resection or lymph node dissection beyond cholecystectomy alone is not
required for polyps without a histologic confirmation or otherwise high suspicion of cancer.
If, however, based on preoperative factors, there is a high suspicion of cancer within the polyp (for example,
a very large single sessile polyp in an older patient), the operation should include a frozen section of the
gallbladder to determine the presence of malignancy. In addition, the technique may include resection of