
Page 61 - Read Online
P. 61
Page 150 Shad. J Transl Genet Genom 2023;7:141-65 https://dx.doi.org/10.20517/jtgg.2023.11
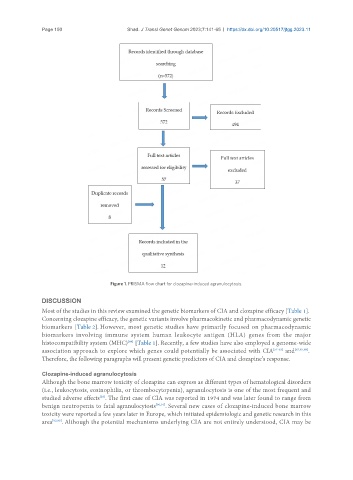
Figure 1. PRISMA flow chart for clozapine-induced agranulocytosis.
DISCUSSION
Most of the studies in this review examined the genetic biomarkers of CIA and clozapine efficacy [Table 1].
Concerning clozapine efficacy, the genetic variants involve pharmacokinetic and pharmacodynamic genetic
biomarkers [Table 2]. However, most genetic studies have primarily focused on pharmacodynamic
biomarkers involving immune system human leukocyte antigen (HLA) genes from the major
[89]
histocompatibility system (MHC) [Table 1]. Recently, a few studies have also employed a genome-wide
association approach to explore which genes could potentially be associated with CIA [51-53] and [62,87,88] .
Therefore, the following paragraphs will present genetic predictors of CIA and clozapine’s response.
Clozapine-induced agranulocytosis
Although the bone marrow toxicity of clozapine can express as different types of hematological disorders
(i.e., leukocytosis, eosinophilia, or thrombocytopenia), agranulocytosis is one of the most frequent and
studied adverse effects . The first case of CIA was reported in 1974 and was later found to range from
[29]
benign neutropenia to fatal agranulocytosis [90,91] . Several new cases of clozapine-induced bone marrow
toxicity were reported a few years later in Europe, which initiated epidemiologic and genetic research in this
area [92,93] . Although the potential mechanisms underlying CIA are not entirely understood, CIA may be