
Page 41 - Read Online
P. 41
Page 325 Casas-Alba et al. J Transl Genet Genom 2022;6:322-32 https://dx.doi.org/10.20517/jtgg.2022.03
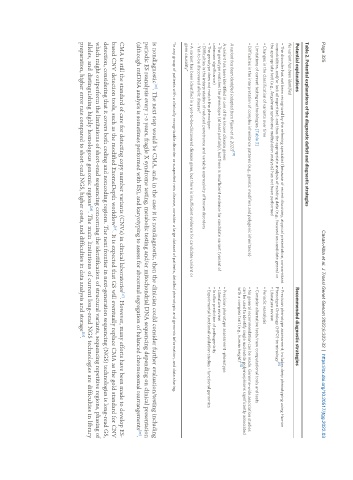
Table 2. Potential explanations of the diagnostic deficit and diagnostic strategies
Potential explanations Recommended diagnostic strategies
No variant has been identified
• The disorder has not been recognized by the referring specialist (because of recent discovery, atypical presentation, concomitant • Precision phenotype assessment; includes deep phenotyping using Human
[11]
comorbidities, and/or lack of expertise), and thus the appropriate analysis of existing data (e.g., focused on candidate genes) or Phenotype Ontology (HPO) terminology
the appropriate test (e.g., Angelman syndrome methylation analysis) has not been performed • Literature review
• Changes in the classification of variants over time • Periodic reanalysis
• Limitations of current testing methodologies [Table 3] • Consider alternative tests/new computational tools and tests
• Difficulties in the interpretation of complex inheritance patterns (e.g., genetic modifiers and polygenic inheritance) • No general recommendation can be made. Genome-wide association studies
can be used to identify single nucleotide polymorphisms significantly associated
with a complex trait (e.g., human height) [12]
[13]
A variant has been identified (adapted from Pijuan et al. 2021)
A variant has been identified in one of the known disease genes: • Precision phenotype assessment -phenotype
• The genotype matches the phenotype (at least partially), but there is insufficient evidence for candidate variant (variant of • Literature review
unknown significance) • In silico prediction of pathogenicity
• The genotype does not match the phenotype: • Experimental functional validation studies - functional genomics
- Difficulties in the interpretation of reduced penetrance and variable expressivity of known disorders
- Yet-to-be discovered allelic disease*
• A variant has been identified in a yet-to-be-discovered disease gene, but there is insufficient evidence for candidate variant or
gene causality*
*In any group of patients with a clinically recognizable disorder or suspected new disease, consider a large dataset of patients, detailed phenotypic and genomic information, and data sharing.
is nondiagnostic . The next step would be CMA, and, in the case it is nondiagnostic, then the clinician could consider further evaluation/testing including
[20]
periodic ES reanalysis every 1-3 years, fragile X syndrome testing, metabolic testing and/or mitochondrial DNA sequencing depending on clinical presentation
(although mtDNA analysis is sometimes performed with ES), and karyotyping to assess for abnormal segregation of balanced chromosomal rearrangements .
[20]
[17]
CMA is still the standard of care for detecting copy number variants (CNVs) in clinical laboratories . However, many efforts have been made to develop ES-
based CNV detection tools, such as the modified ExomeDepth workflow . It is expected that GS will eventually replace CMA as the gold standard for CNV
[19]
detection, considering that it covers both coding and noncoding regions. The next frontier in next-generation sequencing (NGS) technologies is long-read GS,
which might outperform the limitations of short-read sequencing concerning the identification of structural variants, sequencing repetitive regions, phasing of
[23]
alleles, and distinguishing highly homologous genomic regions . The main limitations of current long-read NGS technologies are difficulties in library
preparation, higher error rate compared to short-read NGS, higher costs, and difficulties in data analysis and storage .
[23]