
Page 12 - Read Online
P. 12
Morales et al. J Transl Genet Genom 2022;6:257-65 https://dx.doi.org/10.20517/jtgg.2022.01 Page 263
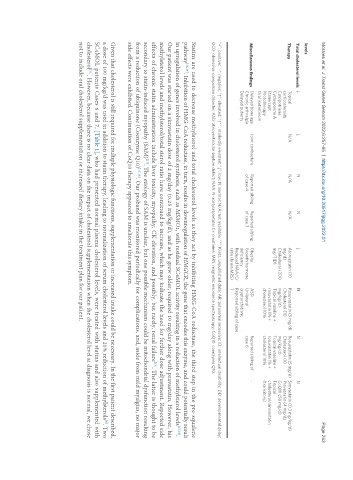
levels
Total cholesterol levels ↓ ↓ N N ↓ N N N
Therapy Topical N/A N/A N/A Atorvastatin (10 Rosuvastatin (5 mg/d) Rosuvastatin (5 mg/d) Simvastatin (0.3 mg/kg/d)
corticosteroids mg/d) Cholesterol (10 Cholesterol (10 Pravastatin (4 mg/d)
Calcipotriene Cholesterol (200 mg/kg/d) mg/kg/d) CoQ10 (50 mg/d)
Cyclosporine A mg/TID) Topical vaseline + Topical vaseline + Topical
Etanercept rosuvastatin 1% + rosuvastatin 1% + cholesterol/simvastatin
Phototherapy cholesterol 10% cholesterol 10% (transitory)
Oral isotretinoin
Miscellaneous findings Delayed bone age Joint contracture Reported sibling Reported sibling Obesity ASD Reported sibling of -
Chronic arthralgia of case 4 of case 3 Growth hormone Unilateral case 6
Delayed puberty deficiency cryptorchidism;
Reduced NAA/Cr Reported sibling of case
ratio (brain MRS) 7
“+”: positive; “-“: negative; “↑”: elevated; “↑↑”: markedly elevated; “↓”: low; N: normal; N/A: not available; “*”: Kratz, unpublished data; AR: autosomal recessive; ID: intellectual disability; DD: developmental delay;
OCD: obsessive-compulsive disorder; ASD: atrioventricular septum defect; NAA: N-acetylaspartate; Cr: creatinine; MRS: magnetic resonance spectroscopy; CoQ10: coenzyme Q10.
Statins are used to decrease methylsterol and total cholesterol levels as they act by inhibiting HMG-CoA reductase, the third step in the pre-squalene
pathway [13,14] . Inhibition of HMG-CoA reductase, in turn, results in downregulation of HMGCR, the gene that encodes this enzyme, and could potentially result
in upregulation of genes involved in cholesterol synthesis, such as MSMO1, with residual SC4MOL activity resulting in a reduction of methylsterol levels [15,16] .
Our patient was started on a simvastatin dose of 2 mg/day (0.25 mg/kg/d), and as he grew older, required 10 mg/day along with pravastatin. However, his
methylsterol levels and methylsterol/total sterol ratio have continued to increase, which may indicate the need for further dose adjustment. Reported side
effects of chronic statin administration include liver toxicity, myopathy, CK elevation, and possibly, but rarely, renal failure . The latter is thought to be
[13]
secondary to statin-induced myopathy (SAM) . The etiology of SAM is unclear, but one possible mechanism could be mitochondrial dysfunction resulting
[17]
from a reduction of ubiquinone (Coenzyme Q10) [17,18] . Our proband was monitored periodically for complications, and, aside from mild myalgias, no major
side effects were exhibited. Continuation of CoQ10 therapy appeared to ameliorate this symptom.
Given that cholesterol is still required for multiple physiologic functions, supplementation or increased intake could be necessary. In the first patient described,
[6]
a dose of 100 mg/kg/d was used in addition to statin therapy, leading to normalization of serum cholesterol levels and 20% reduction of methylsterols . Two
SC4MOL patients Cases 6 and 7, [Table 1], who had presented normal plasma cholesterol levels, were treated with statins and also supplemented with
[11]
cholesterol . However, because there is no clear data on the impact of cholesterol supplementation when the cholesterol level at diagnosis is normal, we chose
not to include oral cholesterol supplementation or increased dietary intake in the treatment plan for our patient.