
Page 105 - Read Online
P. 105
Watson et al. J Transl Genet Genom 2020;4:188-202 I http://dx.doi.org/10.20517/jtgg.2020.31 Page 191
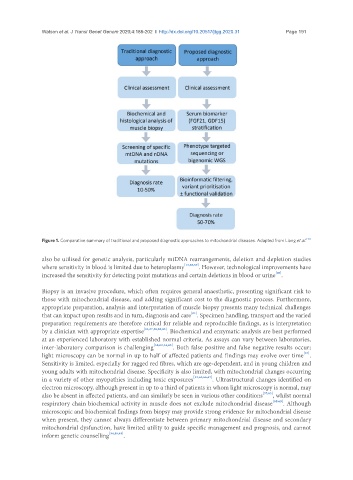
Figure 1. Comparative summary of traditional and proposed diagnostic approaches to mitochondrial diseases. Adapted from Liang et al. [13]
also be utilised for genetic analysis, particularly mtDNA rearrangements, deletion and depletion studies
where sensitivity in blood is limited due to heteroplasmy [13,58,59] . However, technological improvements have
[60]
increased the sensitivity for detecting point mutations and certain deletions in blood or urine .
Biopsy is an invasive procedure, which often requires general anaesthetic, presenting significant risk to
those with mitochondrial disease, and adding significant cost to the diagnostic process. Furthermore,
appropriate preparation, analysis and interpretation of muscle biopsy presents many technical challenges
[61]
that can impact upon results and in turn, diagnosis and care . Specimen handling, transport and the varied
preparation requirements are therefore critical for reliable and reproducible findings, as is interpretation
by a clinician with appropriate expertise [13,37,58,62,63] . Biochemical and enzymatic analysis are best performed
at an experienced laboratory with established normal criteria. As assays can vary between laboratories,
inter-laboratory comparison is challenging [58,62,64,65] . Both false positive and false negative results occur;
[37]
light microscopy can be normal in up to half of affected patients and findings may evolve over time .
Sensitivity is limited, especially for ragged red fibres, which are age-dependent, and in young children and
young adults with mitochondrial disease. Specificity is also limited, with mitochondrial changes occurring
in a variety of other myopathies including toxic exposures [13,63,66,67] . Ultrastructural changes identified on
electron microscopy, although present in up to a third of patients in whom light microscopy is normal, may
also be absent in affected patients, and can similarly be seen in various other conditions [37,63] , whilst normal
respiratory chain biochemical activity in muscle does not exclude mitochondrial disease [68,69] . Although
microscopic and biochemical findings from biopsy may provide strong evidence for mitochondrial disease
when present, they cannot always differentiate between primary mitochondrial disease and secondary
mitochondrial dysfunction, have limited utility to guide specific management and prognosis, and cannot
inform genetic counselling [54,58,63] .