
Page 58 - Read Online
P. 58
Page 6 of 11 Tirelli et al. J Cancer Metastasis Treat 2023;9:20 https://dx.doi.org/10.20517/2394-4722.2022.98
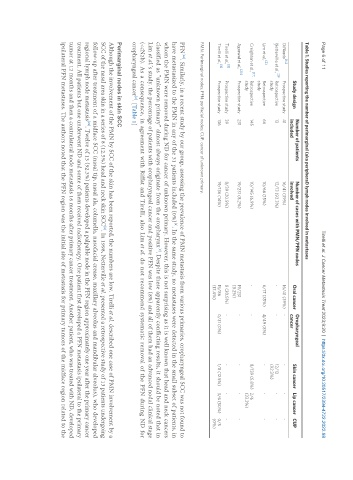
Table 1. Studies reporting the number of perimarginal (aka peripheral) lymph nodes involved in metastases
Number of patients Number of cases with PMN/PFN nodes Oropharyngeal
Study design Oral cancer Skin cancer Lip cancer CUP
included involved cancer
[14]
DiNardo Prospective study 41 16/41 (39%) 16/41 (39%) - - - -
Netterville et al., [29 Retrospective 13 12/13 (92.3%) - - 12/13 - -
]
study (92.3%)
Lim et al., [2] Retrospective 66 10/66 (15%) 6/17 (35%) 4/49 (8%) - - -
study
[17]
Creighton et al., Retrospective 145 10/145 (6.9%) - - 8/139 (5.8%) 2/6
study (33.3%)
[20]
Agarwal et al., Prospective study 231 19/231 (8.2%) 19/231 - - - -
(8.2%)
[8]
Tirelli et al., Prospective study 39 8/39 (20.5%) 8 (20.5%) - - - -
Tirelli et al., [9] Prospective study 136 19/136 (14%) 15/86 0/31 (0%) 1/8 (12.5%) 3/6 (50%) 0/5
(17.4%) (0%)
PMN: Perimarginal nodes; PFN: perifacial nodes; CUP: cancer of unknown primary.
[28]
PFN . Similarly, in a recent study by our group, assessing the prevalence of PMN metastasis from various primaries, oropharyngeal SCC was not found to
have metastasized to the PMN in any of the 31 patients included (0%) . In the same study, no metastases were detected in the small subset of patients, in
[9]
whom the PMN were removed during ND for cancer of unknown primary. However, this is not surprising as it is well known that head and neck cancers
classified as “unknown primary” almost always originate from the oropharynx . Despite these apparently conflicting results, it should be noted that in
[9]
Lim et al.’s study. the percentage of patients with oropharyngeal cancer and positive PFN was low (8%) and all of them had an advanced nodal clinical stage
(<cN2b). As a consequence, in agreement with Riffat and Tirelli, also Lim et al. do not recommend systematic removal of the PFN during ND for
oropharyngeal cancer . [Table 1]
[2]
Perimarginal nodes in skin SCC
Although the involvement of the PMN by SCC of the skin has been reported, the numbers are low. Tirelli et al. described one case of PMN involvement by a
[9]
SCC of the nasal area skin in a series of 8 (12.5%) head and neck skin SCC . In 1998, Netterville et al. presented a retrospective study of 13 patients undergoing
follow-up after treatment of a midface SCC (nasal tip, nasal ala, columella, nasofacial crease, maxillary alveolus and mandibular alveolus), who developed
regional lymph node metastasis . Twelve of 13 (92.3%) patients developed a palpable node in the PFN region approximately one year after the primary cancer
[29]
treatment. All patients but one underwent ND and some of them received radiotherapy. One patient first developed a PFN metastasis ipsilateral to the primary
tumor at 12 months and then a contralateral node metastasis 16 months after primary cancer treatment. Another patient, who was treated with ND, developed
ipsilateral PFN metastases. The authors noted that the PFN region was the initial site of metastasis for primary tumors of the midface region related to the