
Page 27 - Read Online
P. 27
Khan et al. J Cancer Metastasis Treat 2019;5:71 I http://dx.doi.org/10.20517/2394-4722.2019.017 Page 7 of 12
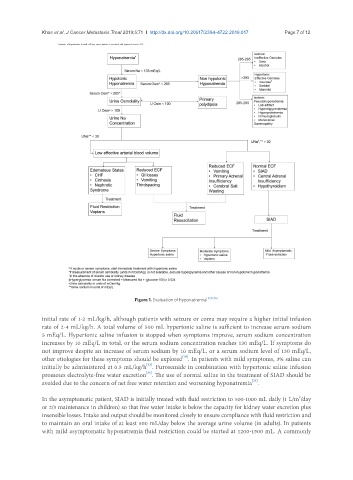
Figure 1. Evaluation of hyponatremia [10,19,46]
initial rate of 1-2 mL/kg/h, although patients with seizure or coma may require a higher initial infusion
rate of 2-4 mL/kg/h. A total volume of 500 mL hypertonic saline is sufficient to increase serum sodium
5 mEq/L. Hypertonic saline infusion is stopped when symptoms improve, serum sodium concentration
increases by 10 mEq/L in total, or the serum sodium concentration reaches 130 mEq/L. If symptoms do
not improve despite an increase of serum sodium by 10 mEq/L, or a serum sodium level of 130 mEq/L,
[10]
other etiologies for these symptoms should be explored . In patients with mild symptoms, 3% saline can
[32]
initially be administered at 0.5 mL/kg/h . Furosemide in combination with hypertonic saline infusion
[33]
promotes electrolyte-free water excretion . The use of normal saline in the treatment of SIAD should be
[33]
avoided due to the concern of net free water retention and worsening hyponatremia .
2
In the asymptomatic patient, SIAD is initially treated with fluid restriction to 500-1000 mL daily (1 L/m /day
or 2/3 maintenance in children) so that free water intake is below the capacity for kidney water excretion plus
insensible losses. Intake and output should be monitored closely to ensure compliance with fluid restriction and
to maintain an oral intake of at least 500 mL/day below the average urine volume (in adults). In patients
with mild asymptomatic hyponatremia fluid restriction could be started at 1200-1500 mL. A commonly