
Page 16 - Read Online
P. 16
Page 4 of 8 Fiordoliva et al. J Cancer Metastasis Treat 2019;5:59 I http://dx.doi.org/10.20517/2394-4722.2019.23
Figure 3. CT scan showing liver metastatization and rectal thickening
A B
C D
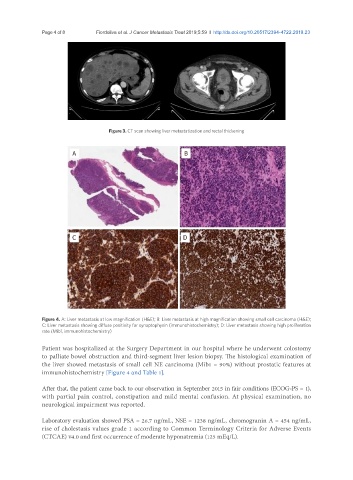
Figure 4. A: Liver metastasis at low magnification (H&E); B: Liver metastasis at high magnification showing small cell carcinoma (H&E);
C: Liver metastasis showing diffuse positivity for synaptophysin (immunohistochemistry); D: Liver metastasis showing high proliferation
rate (Mib1, immunohistochemistry)
Patient was hospitalized at the Surgery Department in our hospital where he underwent colostomy
to palliate bowel obstruction and third-segment liver lesion biopsy. The histological examination of
the liver showed metastasis of small cell NE carcinoma (Mib1 = 90%) without prostatic features at
immunohistochemistry [Figure 4 and Table 1].
After that, the patient came back to our observation in September 2015 in fair conditions (ECOG-PS = 1),
with partial pain control, constipation and mild mental confusion. At physical examination, no
neurological impairment was reported.
Laboratory evaluation showed PSA = 26.7 ng/mL, NSE = 1238 ng/mL, chromogranin A = 454 ng/mL,
rise of cholestasis values grade 1 according to Common Terminology Criteria for Adverse Events
(CTCAE) v4.0 and first occurrence of moderate hyponatremia (125 mEq/L).