
Page 16 - Read Online
P. 16
Page 10 of 17 Spallanzani et al. J Cancer Metastasis Treat 2018;4:28 I http://dx.doi.org/10.20517/2394-4722.2018.31
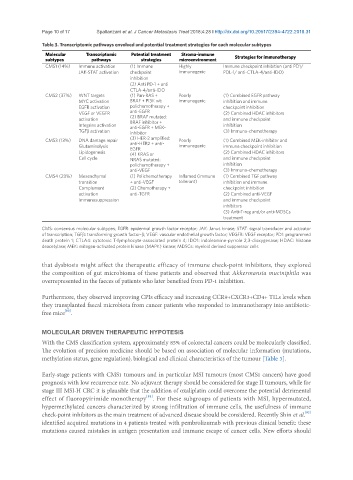
Table 3. Transcriptomic pathways envolved and potential treatment strategies for each molecular subtypes
Molecular Transcriptomic Potential treatment Stroma-immune Strategies for immunotherapy
subtypes pathways strategies microenvironment
CMS1 (14%) Immune activation (1) Immune Highly Immune checkpoint inhibition (anti PD1/
JAK-STAT activation checkpoint immunogenic PDL-1/ anti-CTLA-4/anti-IDO)
inhibition
(2) Anti PD-1 + anti
CTLA-4/anti-IDO
CMS2 (37%) WNT targets (1) Pan-RAS + Poorly (1) Combined EGFR pathway
MYC activation BRAF + PI3K wt: immunogenic inhibition and immune
EGFR activation polichemotherapy + checkpoint inhibition
VEGF or VEGFR anti-EGFR (2) Combined HDAC inhibitors
activation (2) BRAF mutated: and immune checkpoint
BRAF inhibitor +
Integrins activation anti-EGFR + MEK- inhibition
TGFβ activation inhibitor (3) Immuno-chemotherapy
CMS3 (13%) DNA damage repair (3) HER-2 amplified: Poorly (1) Combined MEK-inhibitor and
Glutaminolysis anti-HER2 + anti- immunogenic immune checkpoint inhibition
EGFR
Lipidogenesis (4) KRAS or (2) Combined HDAC inhibitors
Cell cycle NRAS mutated: and immune checkpoint
polichemotherapy + inhibition
anti-VEGF (3) Immuno-chemotherapy
CMS4 (23%) Mesenchymal (1) Polichemotherapy Inflamed (immune (1) Combined TGF pathway
transition + anti-VEGF tollerant) inhibition and immune
Complement (2) Chemotherapy + checkpoint inhibition
activation anti-TGFR (2) Combined anti-VEGF
Immunosuppression and immune checkpoint
inhibitors
(3) Anti-T-reg and/or anti-MDSCs
treatment
CMS: consensus molecular subtypes; EGFR: epidermal growth factor receptor; JAK: Janus kinase; STAT: signal transducer and activator
of transcription; TGFβ: transforming growth factor-β; VEGF: vascular endothelial growth factor; VEGFR: VEGF receptor; PD1: programmed
death protein 1; CTLA4: cytotoxic T-lymphocyte-associated protein 4; IDO1: indoleamine-pyrrole 2,3-dioxygenase; HDAC: histone
deacetylase; MEK: mitogen-activated protein kinase (MAPK) kinase; MDSCs: myeloid derived suppressor cells
that dysbiosis might affect the therapeutic efficacy of immune check-point inhibitors, they explored
the composition of gut microbioma of these patients and observed that Akkermansia muciniphila was
overrepresented in the faeces of patients who later benefited from PD-1 inhibition.
Furthermore, they observed improving CPIs efficacy and increasing CCR9+CXCR3+CD4+ TILs levels when
they transplanted faecal microbiota from cancer patients who responded to immunotherapy into antibiotic-
[80]
free mice .
MOLECULAR DRIVEN THERAPEUTIC HYPOTESIS
With the CMS classification system, approximately 85% of colorectal cancers could be molecularly classified.
The evolution of precision medicine should be based on association of molecular information (mutations,
methylation status, gene regulation), biological and clinical characteristics of the tumour [Table 3].
Early-stage patients with CMS1 tumours and in particular MSI tumours (most CMS1 cancers) have good
prognosis with low recurrence rate. No adjuvant therapy should be considered for stage II tumours, while for
stage III MSI-H CRC it is plausible that the addition of oxaliplatin could overcome the potential detrimental
[81]
effect of fluoropyirimide monotherapy . For these subgroups of patients with MSI, hypermutated,
hypermethylated cancers characterized by strong infiltration of immune cells, the usefulness of immune
[82]
check-point inhibitors as the main treatment of advanced disease should be considered. Recently Shin et al.
identified acquired mutations in 4 patients treated with pembrolizumab with previous clinical benefit: these
mutations caused mistakes in antigen presentation and immune escape of cancer cells. New efforts should