
Page 802 - Read Online
P. 802
Calabrò et al. Hepatoma Res 2020;6:69 I http://dx.doi.org/10.20517/2394-5079.2020.63 Page 5 of 9
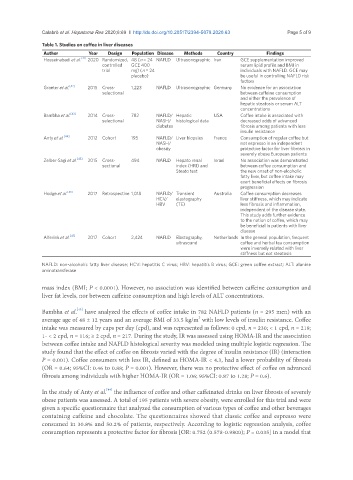
Table 1. Studies on coffee in liver diseases
Author Year Design Population Disease Methods Country Findings
Hosseinabadi et al. [41] 2020 Randomized, 48 (n = 24 NAFLD Ultrasonographic Iran GCE supplementation improved
controlled GCE 400 serum lipid profile and BMI in
trial mg) (n = 24 individuals with NAFLD. GCE may
placebo) be useful in controlling NAFLD risk
factors
Graeter et al. [42] 2015 Cross- 1,223 NAFLD Ultrasonographic Germany No evidence for an association
selectional between caffeine consumption
and either the prevalence of
hepatic steatosis or serum ALT
concentrations
Bambha et al. [43] 2014 Cross- 782 NAFLD/ Hepatic USA Coffee intake is associated with
selectional NASH/ histological data decreased odds of advanced
diabetes fibrosis among patients with less
insulin resistance
Anty et al. [44] 2012 Cohort 195 NAFLD/ Liver biopsies France Consumption of regular coffee but
NASH/ not espresso is an independent
obesity protective factor for liver fibrosis in
severely obese European patients
Zelber-Sagi et al. [45] 2015 Cross- 494 NAFLD Hepato renal Israel No association was demonstrated
sectional index (HRI) and between coffee consumption and
Steato test the new onset of non-alcoholic
fatty liver, but coffee intake may
exert beneficial effects on fibrosis
progression
Hodge et al. [46] 2017 Retrospective 1,018 NAFLD/ Transient Australia Coffee consumption decreases
HCV/ elastography liver stiffness, which may indicate
HBV (TE) less fibrosis and inflammation,
independent of the disease state.
This study adds further evidence
to the notion of coffee, which may
be beneficial in patients with liver
disease
Alferink et al. [47] 2017 Cohort 2,424 NAFLD Elastography, Netherlands In the general population, frequent
ultrasound coffee and herbal tea consumption
were inversely related with liver
stiffness but not steatosis
NAFLD: non-alcoholic fatty liver disease; HCV: hepatitis C virus; HBV: hepatitis B virus; GCE: green coffee extract; ALT: alanine
aminotransferase
mass index (BMI; P < 0.0001). However, no association was identified between caffeine consumption and
liver fat levels, nor between caffeine consumption and high levels of ALT concentrations.
[43]
Bambha et al. have analyzed the effects of coffee intake in 782 NAFLD patients (n = 295 men) with an
average age of 48 ± 12 years and an average BMI of 33.5 kg/m with low levels of insulin resistance. Coffee
2
intake was measured by cups per day (cpd), and was represented as follows: 0 cpd, n = 230; < 1 cpd, n = 219;
1- < 2 cpd, n = 116; ≥ 2 cpd, n = 217. During the study, IR was assessed using HOMA-IR and the association
between coffee intake and NAFLD histological severity was modeled using multiple logistic regression. The
study found that the effect of coffee on fibrosis varied with the degree of insulin resistance (IR) (interaction
P = 0.001). Coffee consumers with less IR, defined as HOMA-IR < 4.3, had a lower probability of fibrosis
(OR = 0.64; 95%CI: 0.46 to 0.88; P = 0.001). However, there was no protective effect of coffee on advanced
fibrosis among individuals with higher HOMA-IR (OR = 1.06; 95%CI: 0.87 to 1.28; P = 0.6).
[44]
In the study of Anty et al. the influence of coffee and other caffeinated drinks on liver fibrosis of severely
obese patients was assessed. A total of 195 patients with severe obesity, were enrolled for this trial and were
given a specific questionnaire that analyzed the consumption of various types of coffee and other beverages
containing caffeine and chocolate. The questionnaires showed that classic coffee and espresso were
consumed in 30.8% and 50.2% of patients, respectively. According to logistic regression analysis, coffee
consumption represents a protective factor for fibrosis [OR: 0.752 (0.578-0.9800); P = 0.035] in a model that